


The 57th Annual Congress of the International Society of Pediatric Oncology (SIOP) was held from October 20-23, 2025, in Amsterdam, the Netherlands.
Venkatraman Radhakrishnan, Associate Professor of Medical and Pediatric Oncology at Chennai Cancer Institute, shared some key highlights from the SIOP Congress:
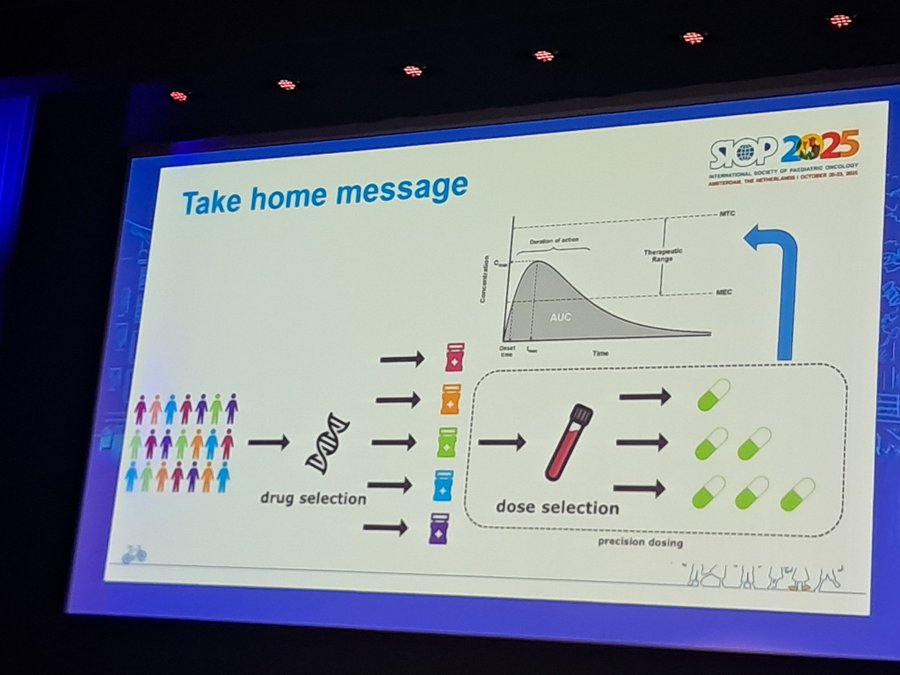
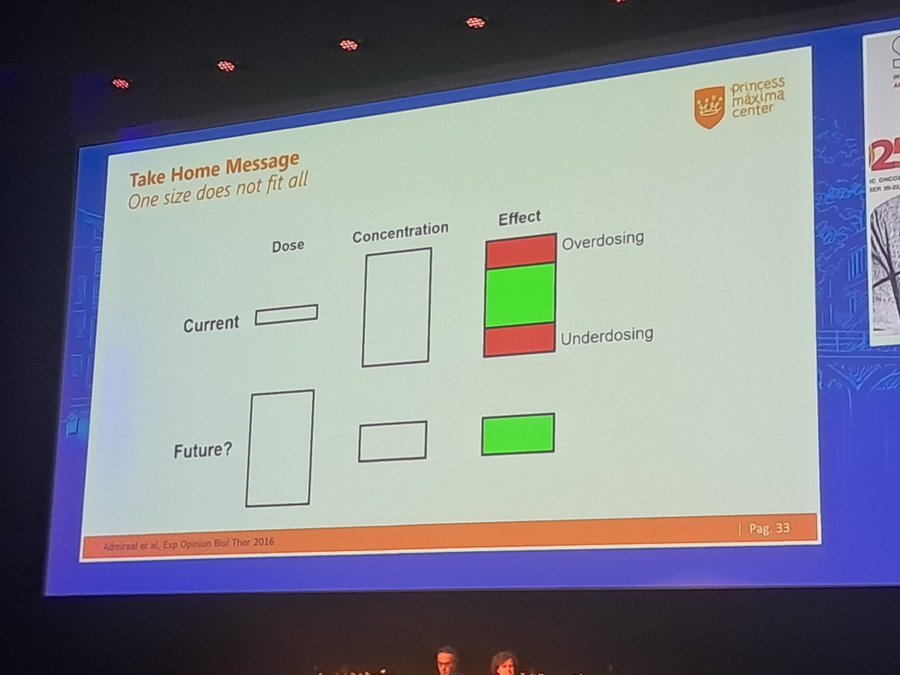
“Precision medicine cannot be possible without precision dosing.
The right drug dose to the right patient at the right time. Even more important in Children. Therapeutic drug monitoring should be the standard of care.”

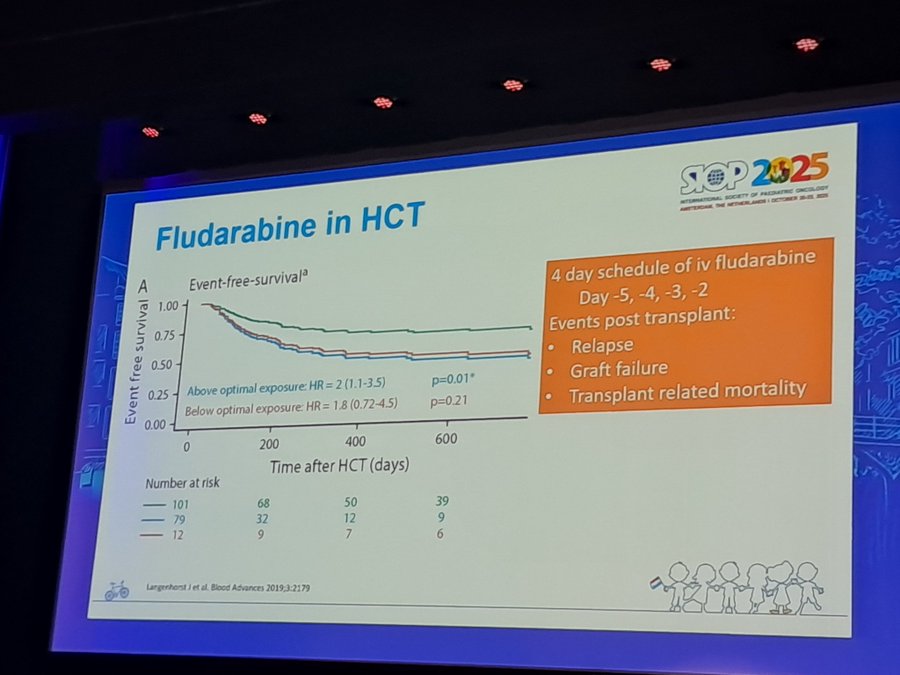
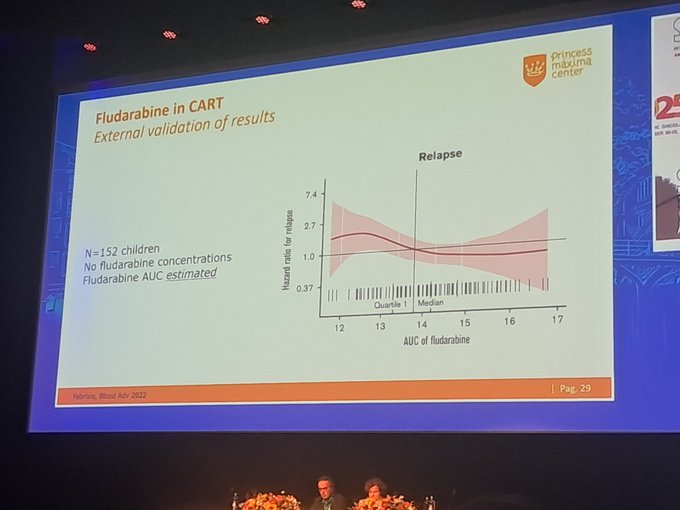
“Drugs we don’t think about, levels like Doxorubicin and Fludarabine have wide variation in drug levels. Fludarabine low levels increased relapse, and high levels more treatment-related mortality in transplant. Important to be between both in the therapeutic range.”

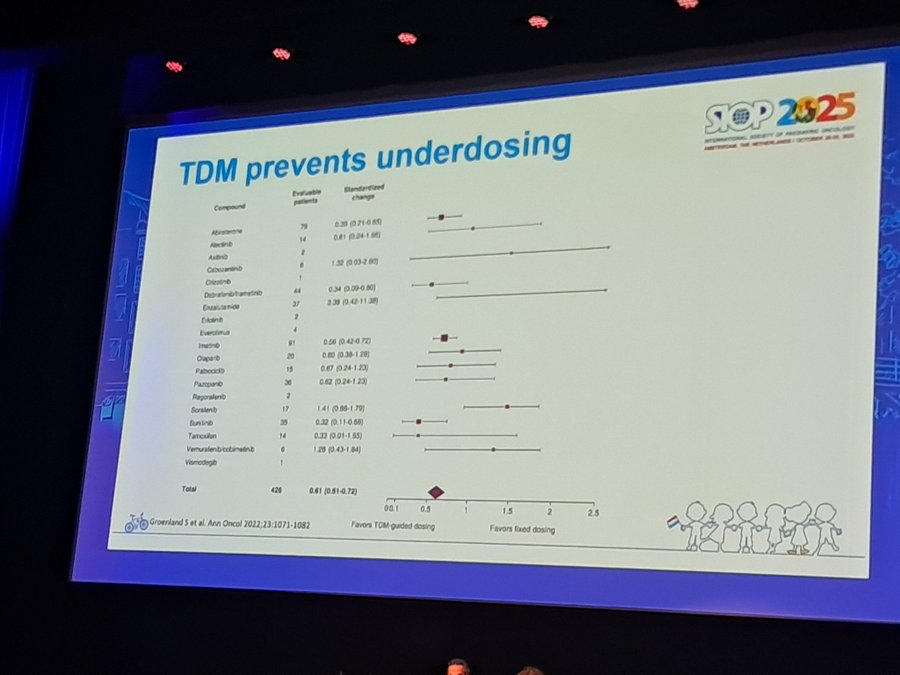
“Even targeted treatment that has a fixed dose benefits from therapeutic drug monitoring and dosing. Look at the Alectinib drug monitoring and outcome. TDM prevents underdosing for most TKI but can be problematic for drugs like Cabozantinib.”

“The future is a genomic passport. While genome sequencing is used to identify drug metabolism in individuals.”

“To conclude, the future is person-listed drug dosing.”

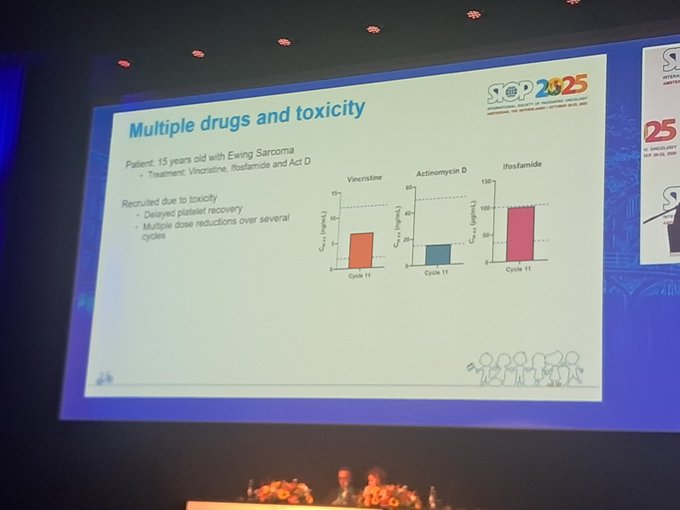
“Therapeutic drug monitoring in pediatric oncology: UK experience. We all have children for whom we reduce doses of all drugs because of toxicity. TDM helps us to identify the drug that is causing the toxicity. Thereby not reducing the Efficacy of other drugs.”

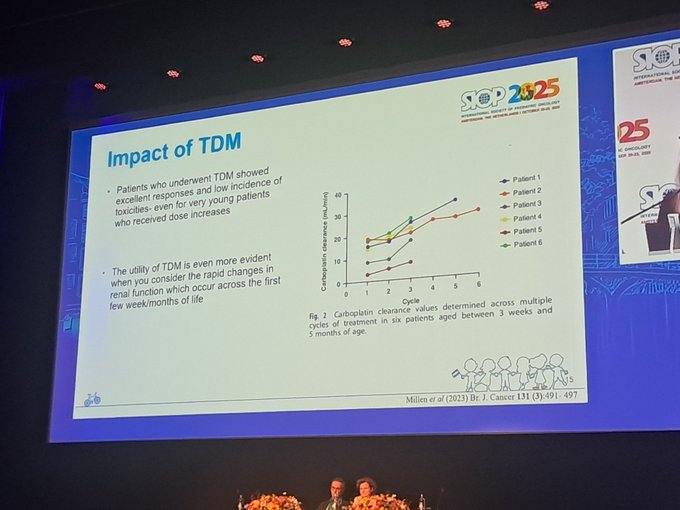
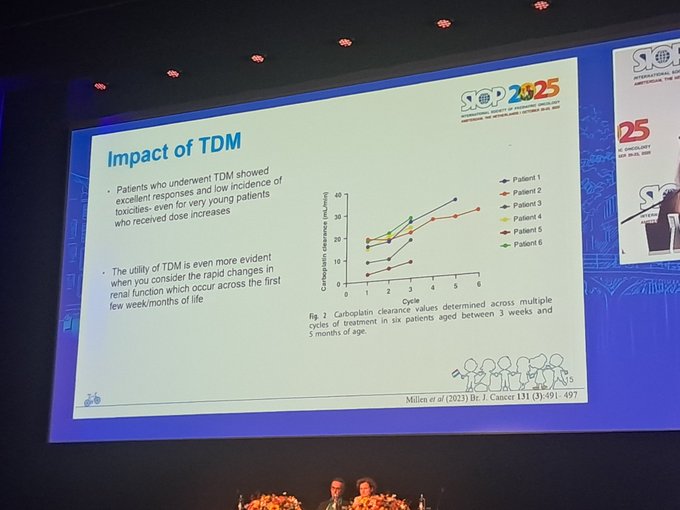
“Children with retinoblastoma who had carboplatin level monitoring have better outcomes.
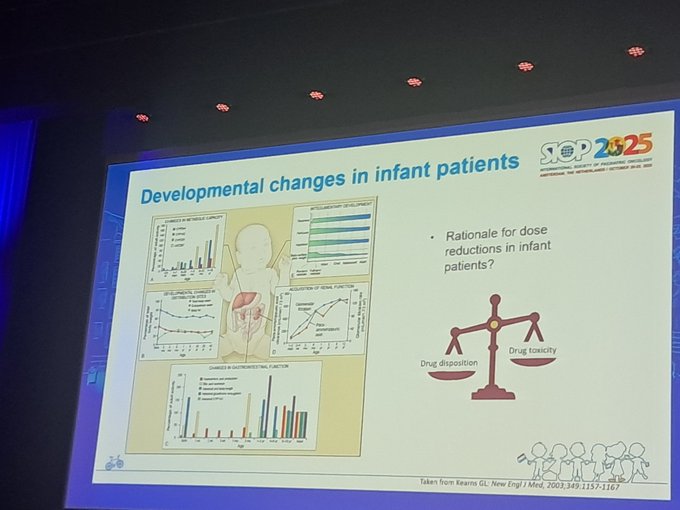
Infants benefit a lot from TDM as there is a wide variation in drug metabolism.”

“Therapeutic drug monitoring in BMT.
So many conditioning regimens. No standard of care. A Centre in the UK decided to have a single regimen for all transplants.
Fludarabine, Anti-thymocyte globulin, and busulphan FLuBuATG and did TDM.”

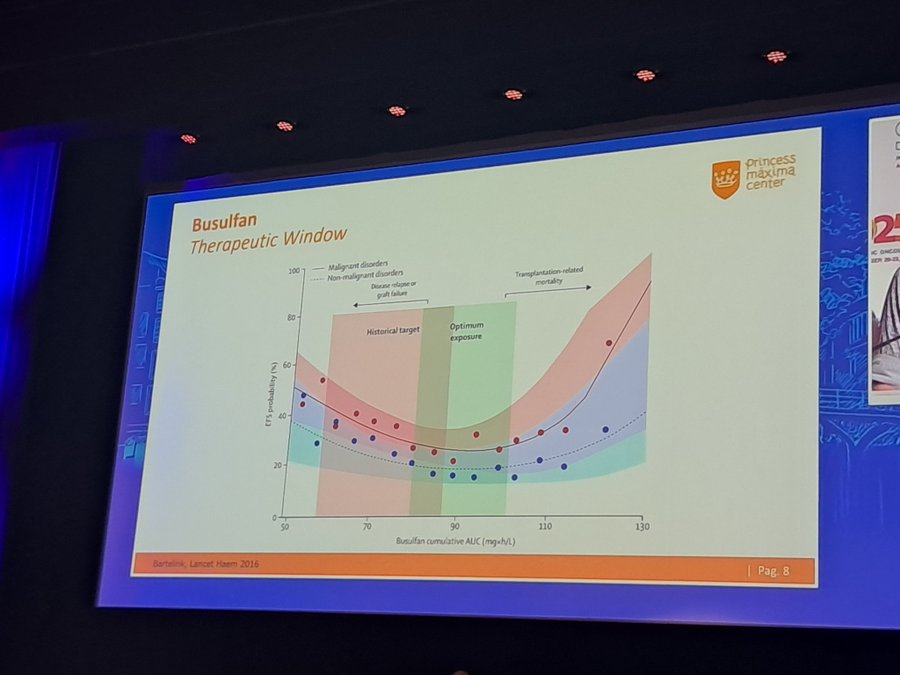
“Busulphan historical perspective.”

“Busulphan metabolism is glutathione-dependent. It has a narrow therapeutic index.”

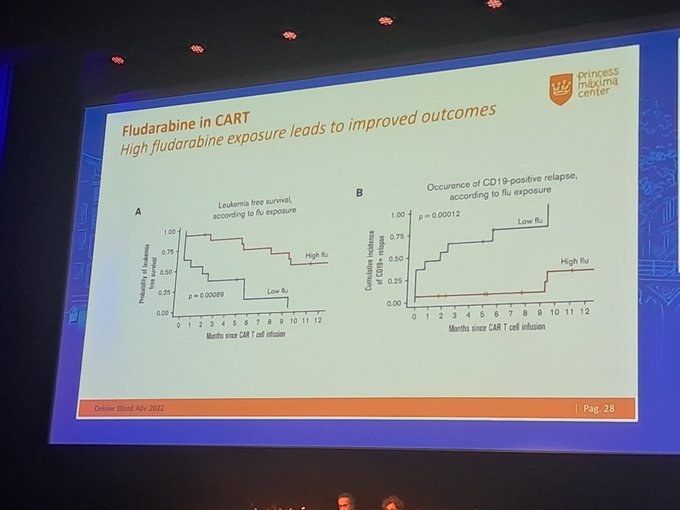
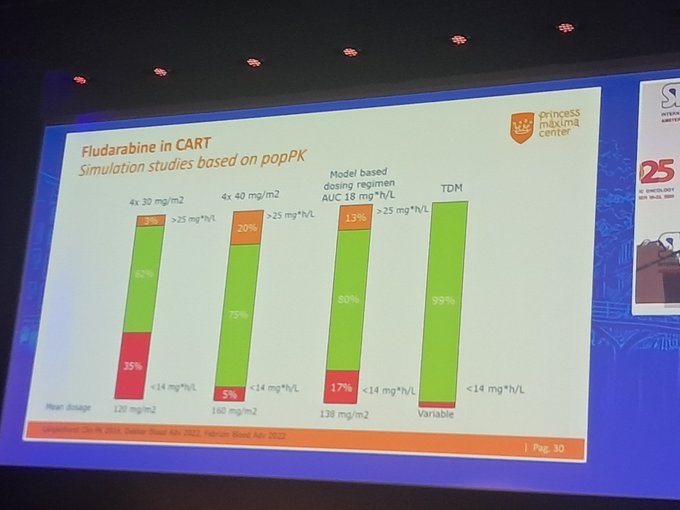
“Importance of Fludarabine conditioning dose with CART. TDM is associated with better outcomes than weight-based dosing.”

“Conclusion: not fixed dose but variable dose based on TDM improves efficacy and outcome.”

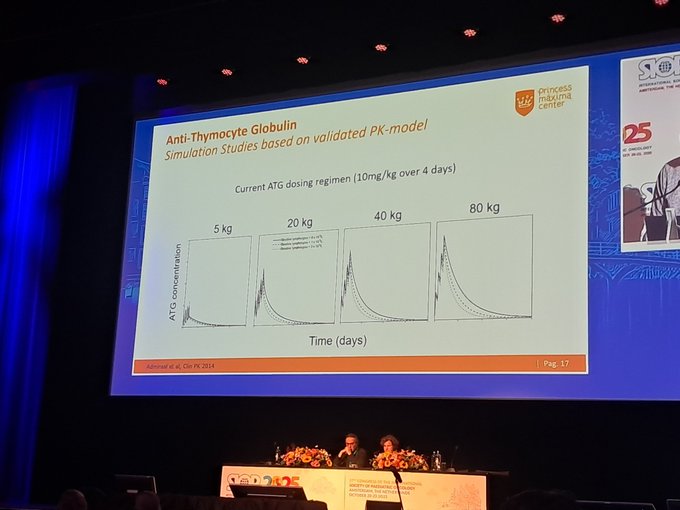
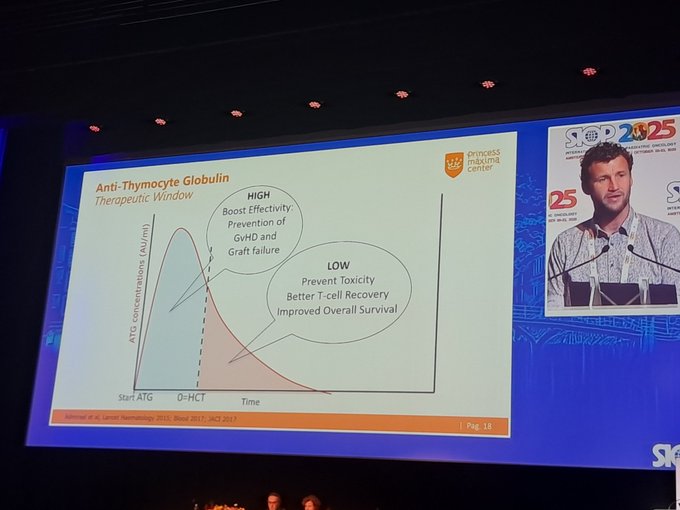
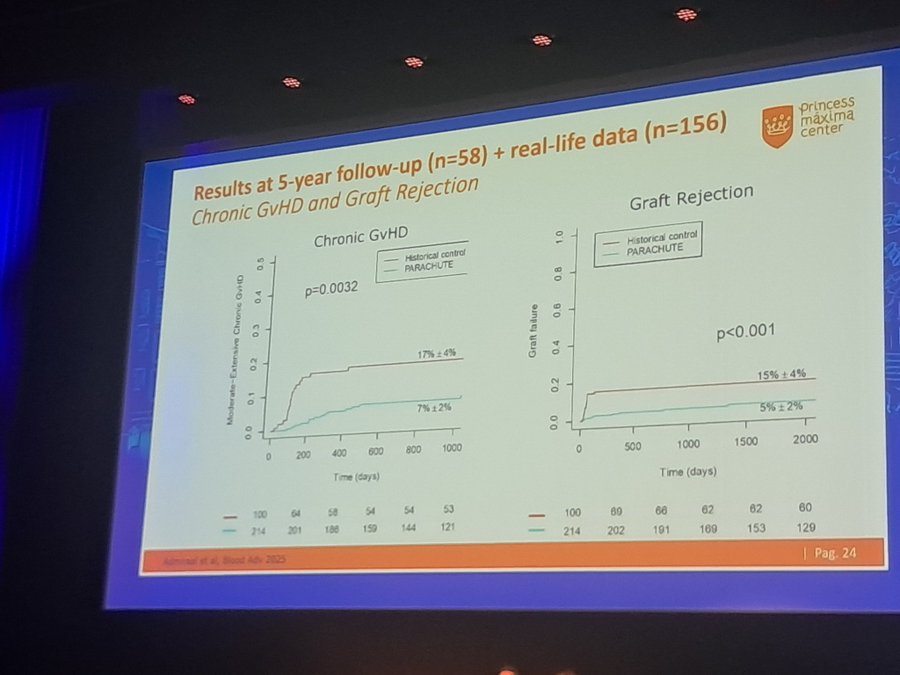
“Next, let’s talk about ATG. The standard dose is 10mg/kg; however, this dose produces lower levels in children and low body weight. ATG dose should be based on weight, lymphocyte count, and cell source. High levels pre-stem cell infusion and low levels post infusion.”

“Using TDM for ATG improves survival, reduces relapses, and GVHD.”

“Model based dosing for ATG.”

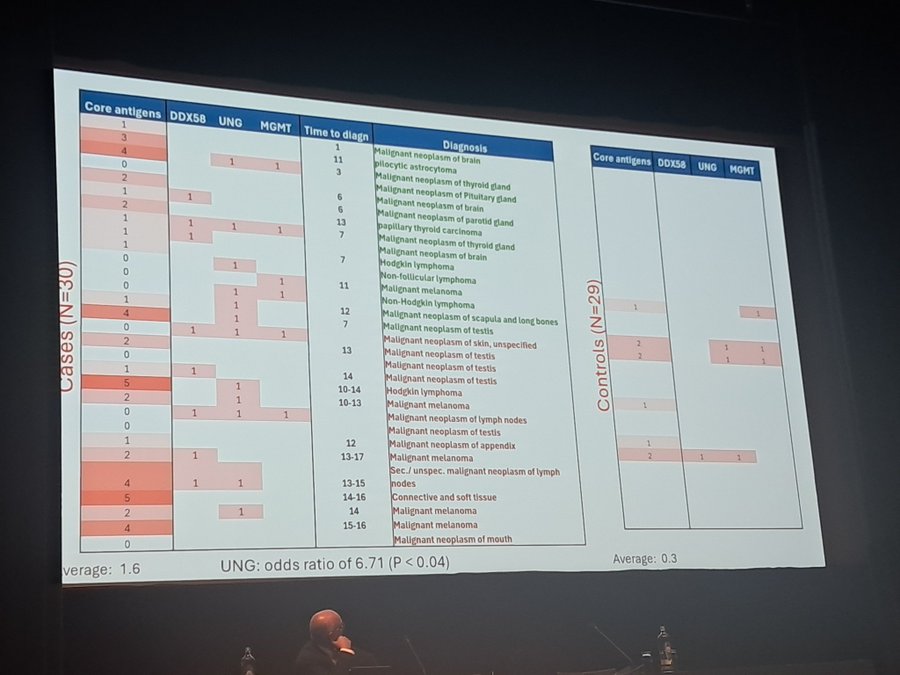
“Do auto antibodies predispose to Cancer? Maybe.
UNG antigen and autoantibody antibody more common in those with cancer than in controls. However need a sample before the detection of the sample to prove the presence of auto antibodies.”

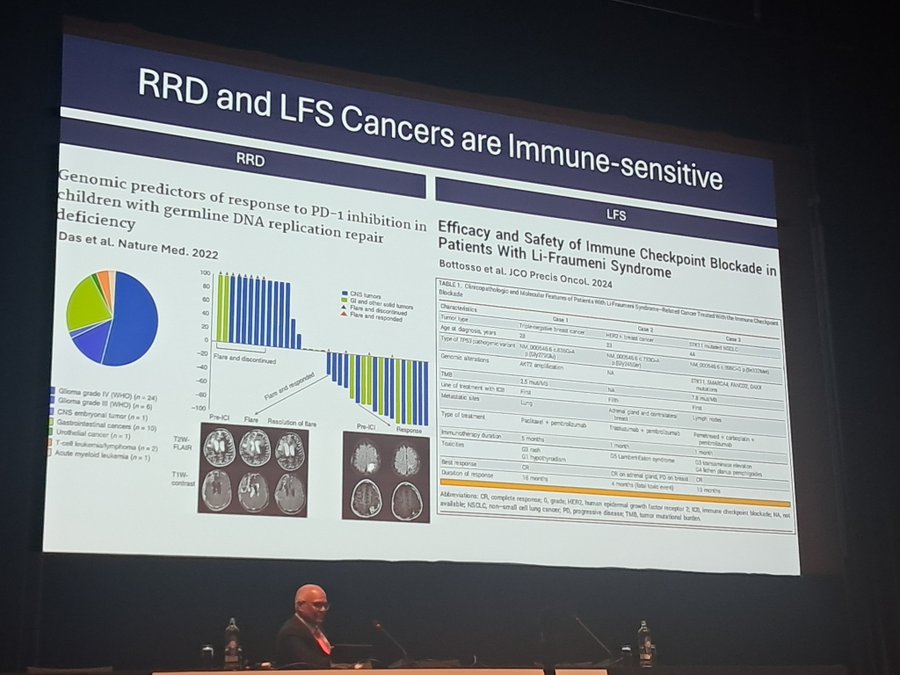
“Surveillance improves outcomes in Li Fraummeni syndrome and Replication Repair Deficit syndromes. These cancers are sensitive to immunotherapy.”

“MEK inhibitors adverse events. Mainly skin and hair changes.”

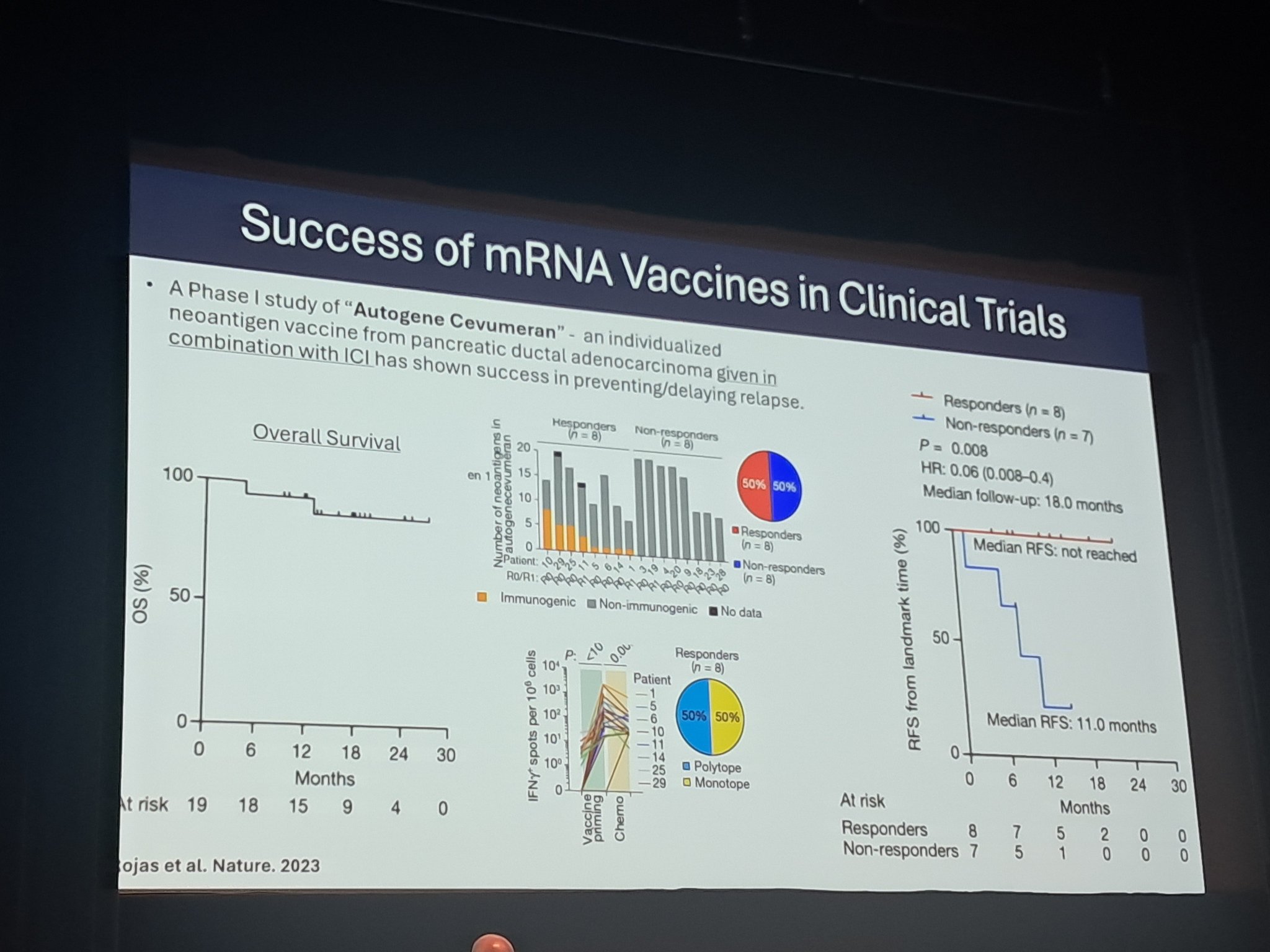
“Are RNA-based cancer vaccines the cure? Good data in pancreatic cancer.”

“Early detection of cancer in Li Fraummeni syndrome using liquid biopsy.”

“Virtual agent tumor board. AI on cancer. ML6.
Use it before the human tumor board.”

“Can we create a digital twin of oncology experts? AI can make it possible. The twin will join tumor boards across the world. This sounds crazy, but it is happening now in Google.”


“Oncologists, you will not be replaced by AI. You will be replaced by someone using AI.”
“Future of patient care. Google Capricorn. Copy-paste your patient data, including lab data. It will read 14 million papers. Then give your opinion.”

“RNA seq identified Notch fusion in T ALL. Poor prognostic factor. Something not important yet doesn’t mean it is not relevant in the future. Not identified by classical FISH.”

“Princess maxima standard of care for molecular diagnostics for pediatric cancers.”

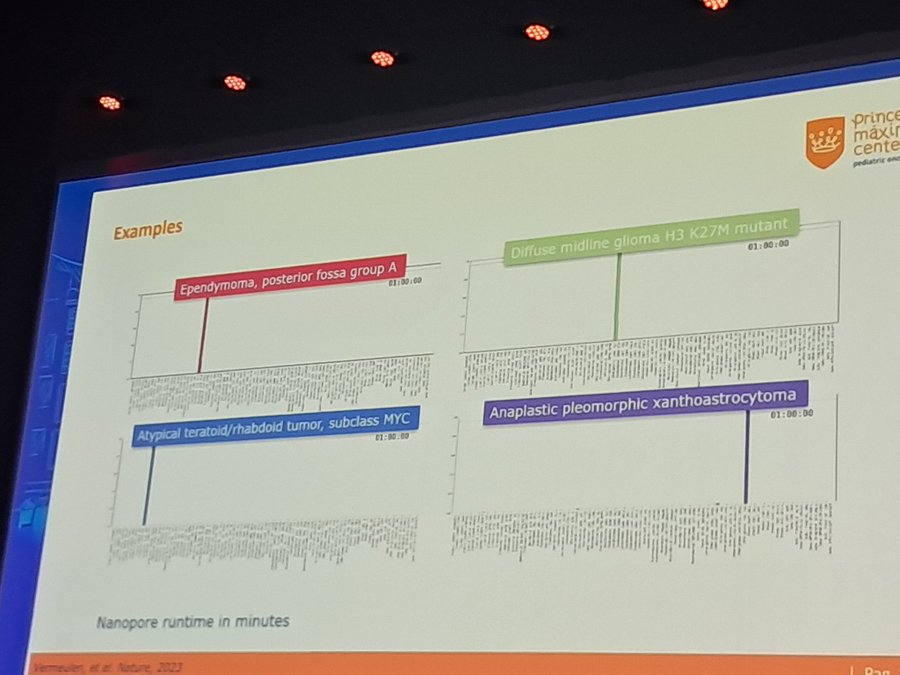
“Future of Molecular Diagnostics. Nanopore sequencing. Fast real-time.”

“Nanopore for better diagnosis of CNS tumour during surgery.”

“Nanopore decides how much you want to sequence.”

“What is a liquid biopsy?”

“Applications of cell-free DNA.”

“How to analyze cell-free DNA.”

“Work flow of cell-free DNA analysis.”

“Cell-free DNA high in pediatric cancers.”

“Use of cell-free DNA to diagnose pediatric Wilms tumor.”


“Brain tumor.”

“Cf DNA identifies neuroblastoma relapse before clinical manifestation and identifies new mutations.”

“Clonal hematopoiesis is age related change in the genome from the germ line due to external stimuli. Chemotherapy can also cause it. It is precancerous.”

“What can you do with liquid biopsy in pediatric cancers?”

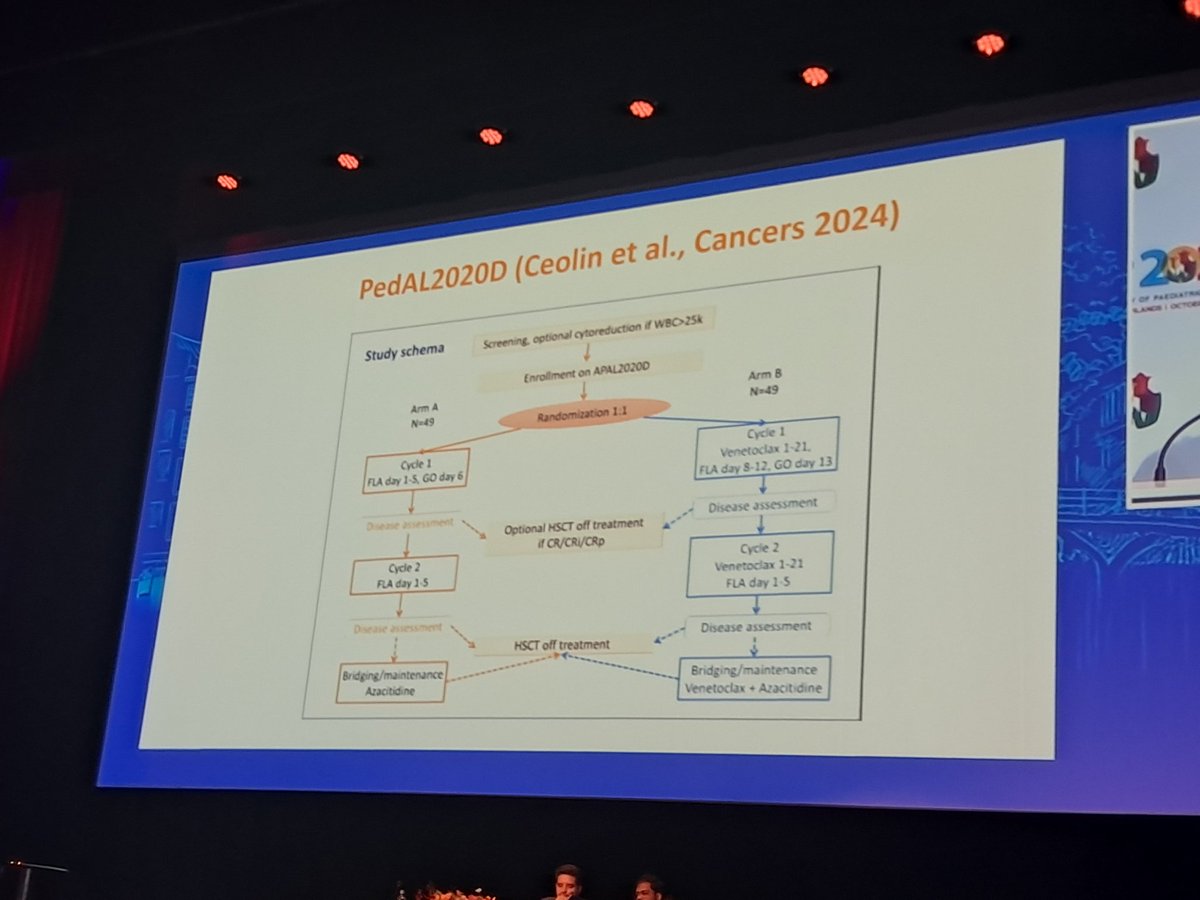
“Treatment of Pediatric AML is complex, even more in the global South.”

“Targeted treatment in AML.”

“Venetoclax in pediatric AML.”

“2 or 3 doses of myelotarg better than 1.”

“FLT3 inhibitors in pediatric AML.”

“Quizartinib doesn’t work in FLT3 TKD mutation.”

“Menin inhibitors in pediatric AML.”

“Pediatric low-grade glioma. Most common pediatric brain tumor. Frequent recurrences. MAPK pathway activated.”

“BRAF inhibitors.”

“Gene fusions in pediatric brain tumors. Rare. NTREK ROoS ALK. Younger age.”

“Sonic Hedge Hog pathway inhibitors lead to premature growth plate fusion. Similar FGFR inhibitors lead to slipped femoral epiphysis. Targeted therapy toxicity in children can be different from adults.”
“MEK inhibitors can lead to weight gain in pediatric brain tumors.”
More posts featuring Venkatraman Radhakrishnan on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}