


The Annual Meeting of the American Society of Clinical Oncology (ASCO) remains one of the most important gatherings in global oncology, bringing together clinicians, researchers, and industry leaders to share the latest developments in cancer care. ASCO 2026 featured practice-changing data, innovative treatment strategies, and new research findings across a wide range of malignancies.
Throughout the meeting, we tracked key presentations, expert commentary, and conversations from the oncology community, and compiled 25 must-read posts from Day 2 of ASCO 2026.
Conquer Cancer, the ASCO Foundation:
“During the American Society of Clinical Oncology (ASCO) Annual Meeting in Chicago this morning, ASCO President Dr. Eric Small shared in his presidential address the importance of the future of discovery in cancer. As a part of that conversation, he urged attendees to make a donation to Conquer Cancer so the cycle of launching careers in research can continue to pave the future of discoveries.
You can also help in this effort by making a donation.”

“One of the most thought-provoking questions during the AI in Oncology Panel Discussion organized by OncoDaily with the sponsorship of ZS wasn’t about what AI can do, it was about what we might lose if we’re not careful.
As AI becomes increasingly integrated into cancer care, how do we preserve critical thinking, human judgment, and the patient experience? How do we ensure that AI supports clinicians rather than replacing the reasoning and empathy that patients rely on?
The panel highlighted an important point: the conversation shouldn’t be about choosing between AI and humans. It should be about using AI responsibly, demanding transparency, and ensuring that technology helps us deliver better, safer, and more accessible care.
A timely discussion as oncology continues to navigate one of the most transformative technological shifts in its history.”

“So excited to co-chair the Pediatric Oncology session at American Society of Clinical Oncology (ASCO) 2026 with Dr. Raya Saab.
This field may be small, but the people in it are incredibly dedicated.
Happy to seeing pediatric oncology represented on the ASCO stage.”

“Honored to have our work on uncommon compound EGFR mutations recognized as a top poster at the ASCO Resident and Med Student Forum! A massive thank you to my incredible mentors Sandip Patel and Tali Azenkot for their guidance and support.”

“ALND indications in 2026 per Boughey at ASCO26
- IBC
- 3+ positive SLNs
- cN2a/cN3 upfront and after NAC, persistent nodal disease or matted nodes at presentation.
- SLN+ (ypN+) still pending A11202 and TAXIS.”

Tom Powles:
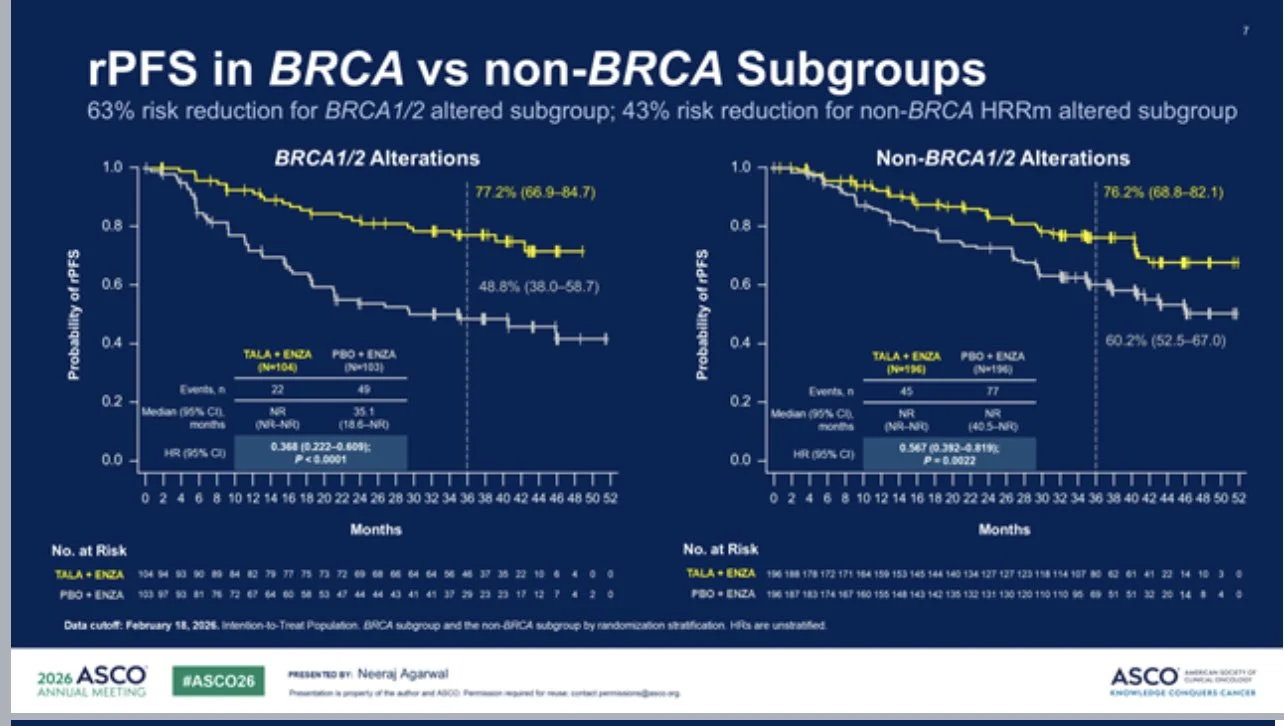
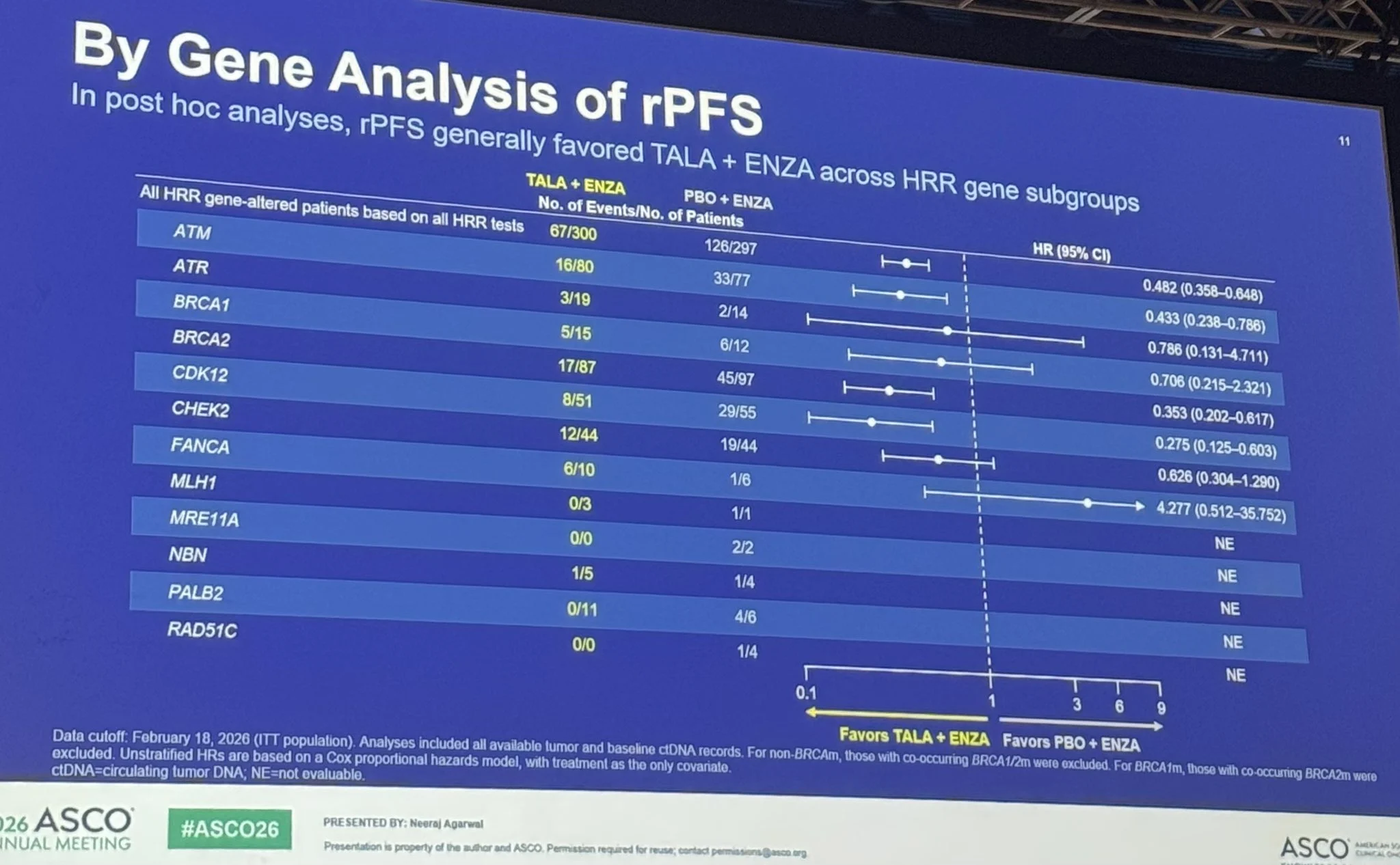
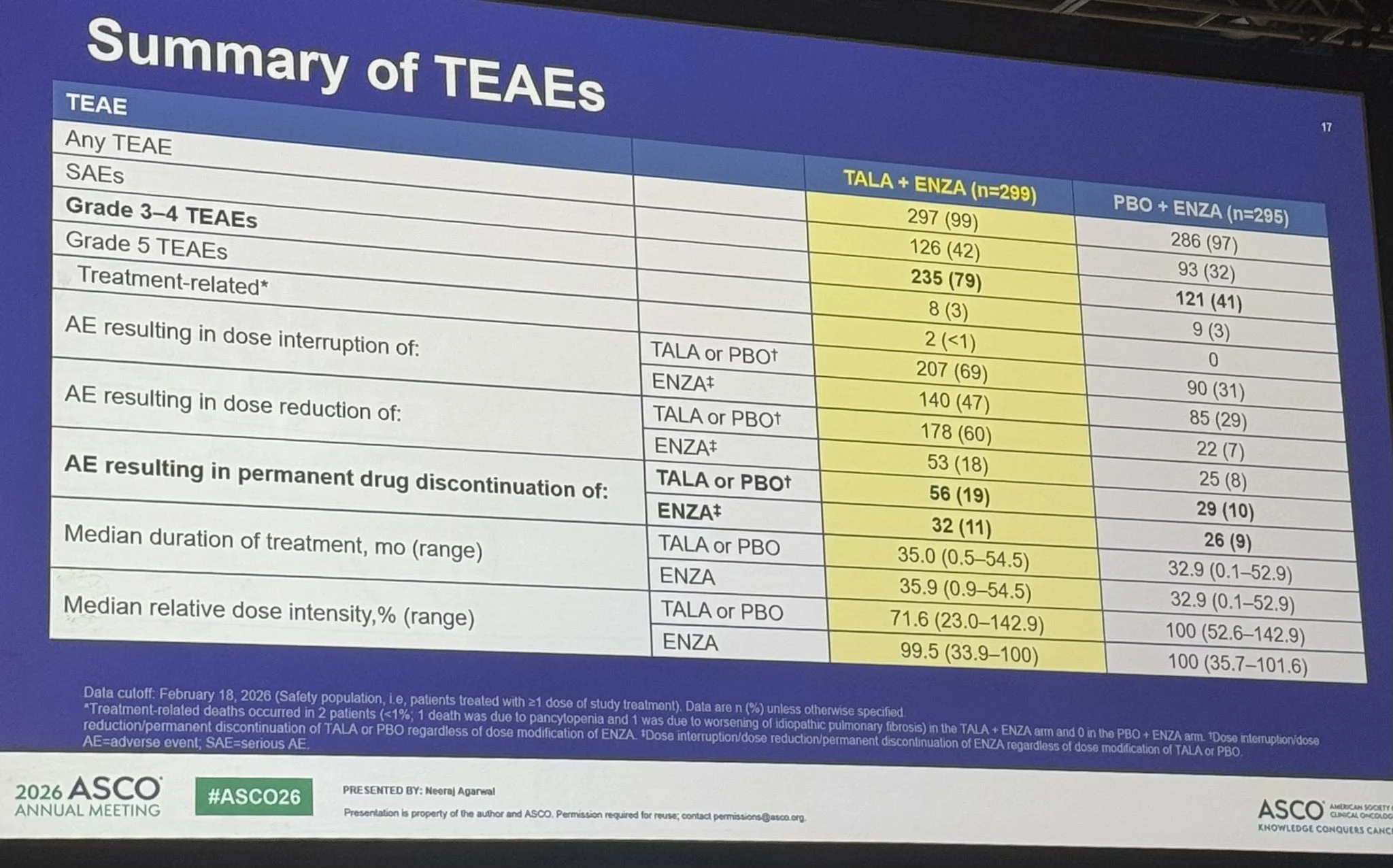
“TALAPRO-3: talazoparib + enzalutamide in HRR-altered mCSPC prostate looks the most impressive PARPi data to date. Efficacy in the non-BRCA HRR population is impressive IMO. Long term treatment is associated with long term side effects.”

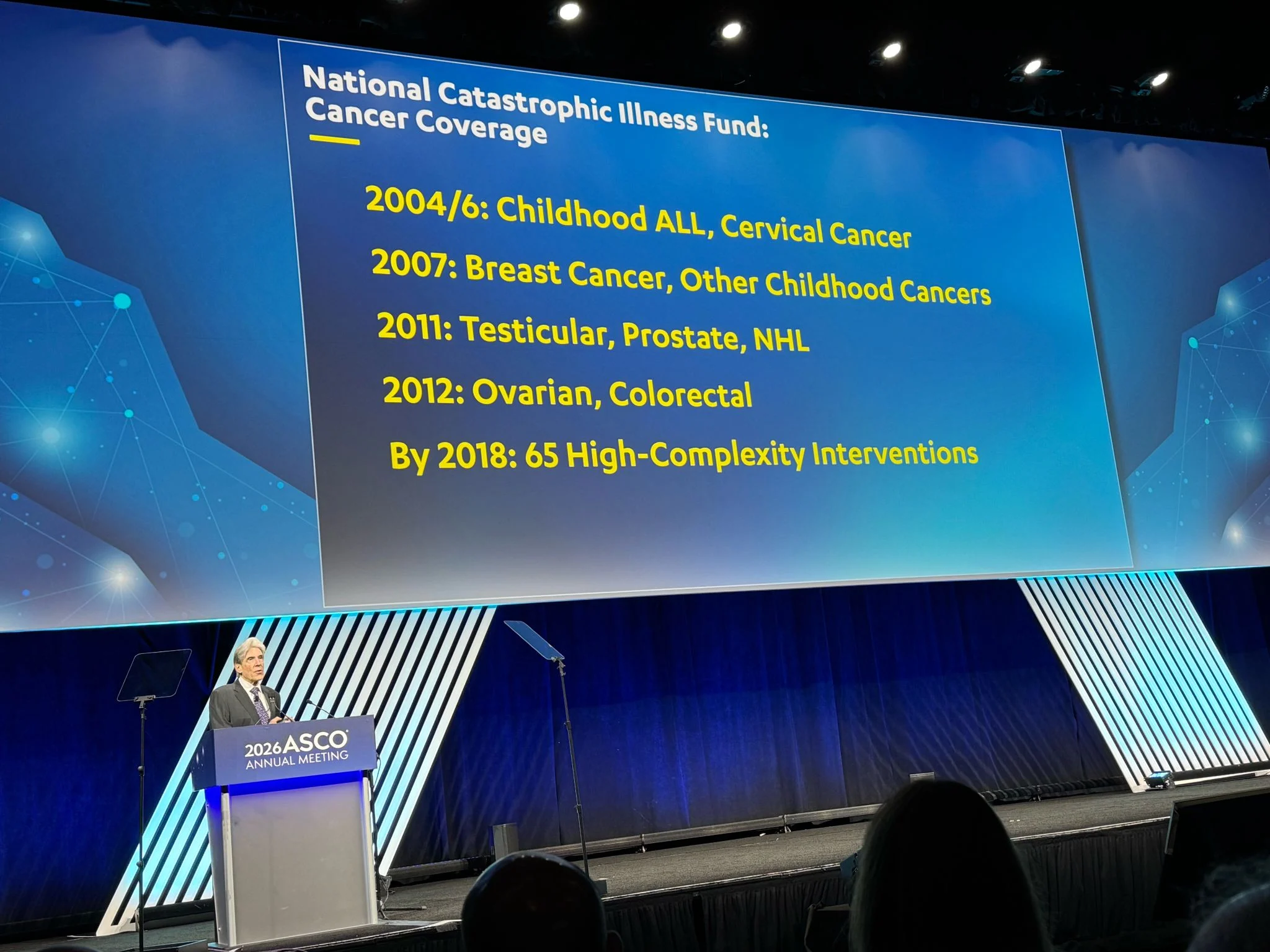
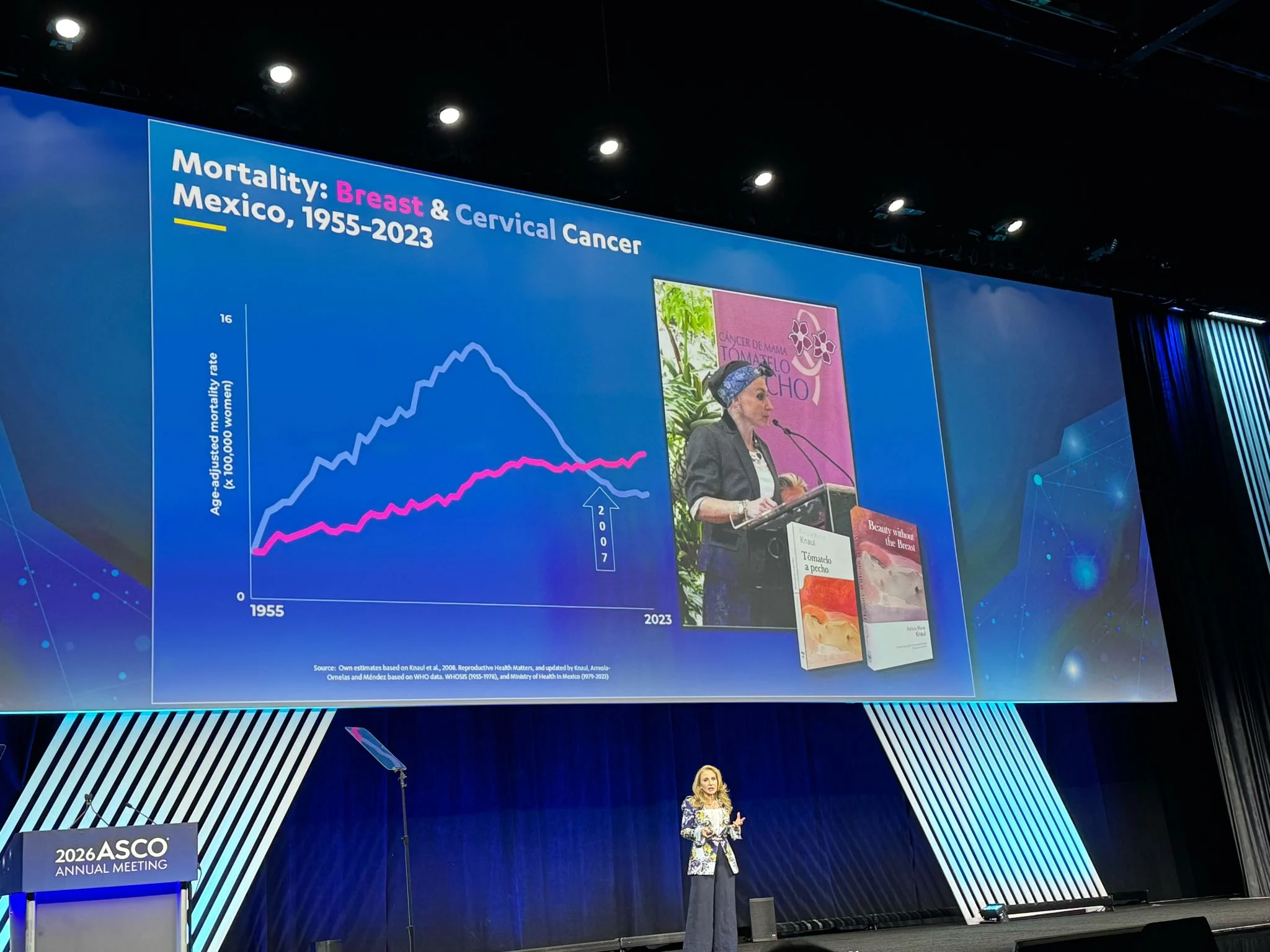
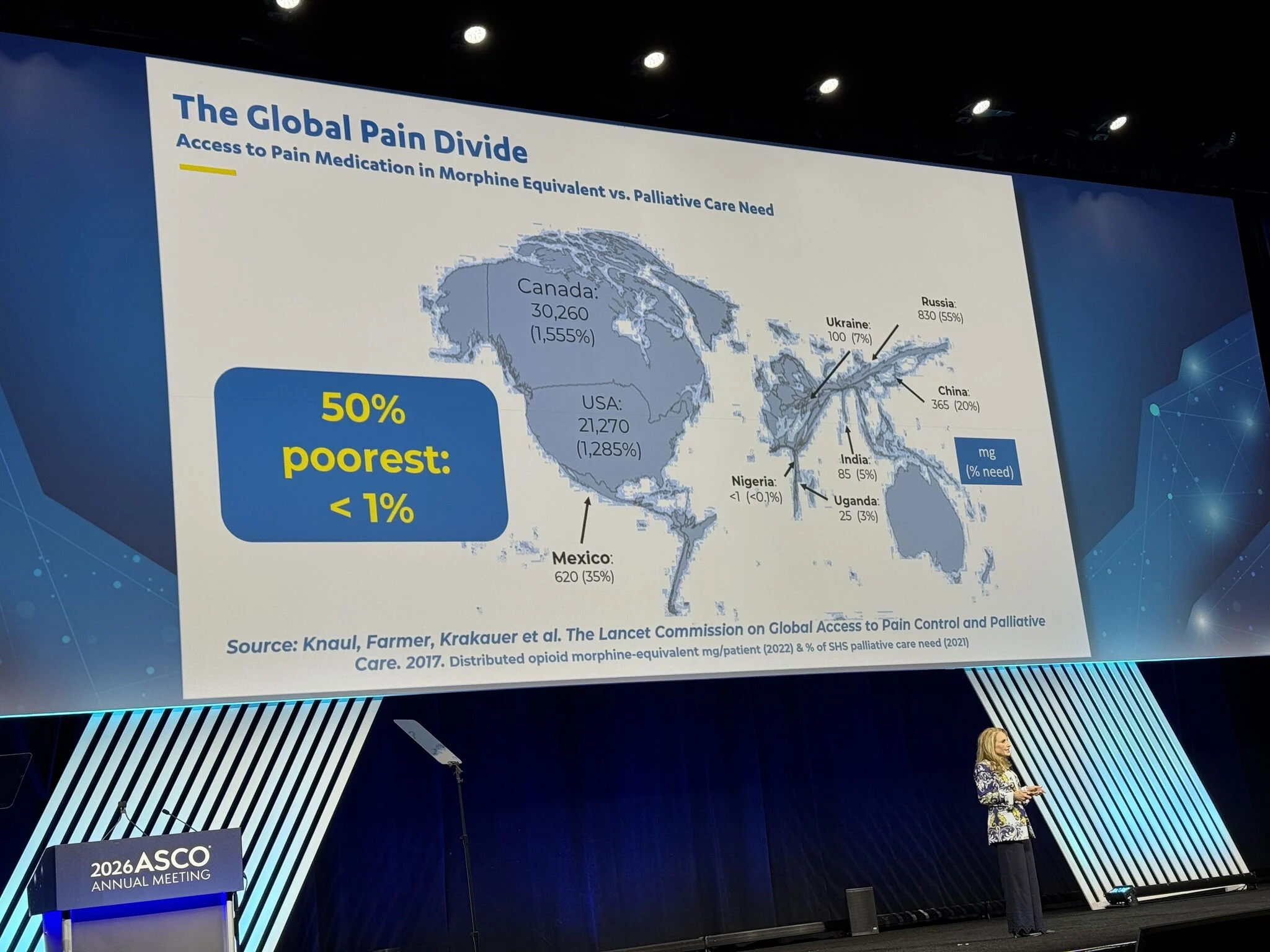
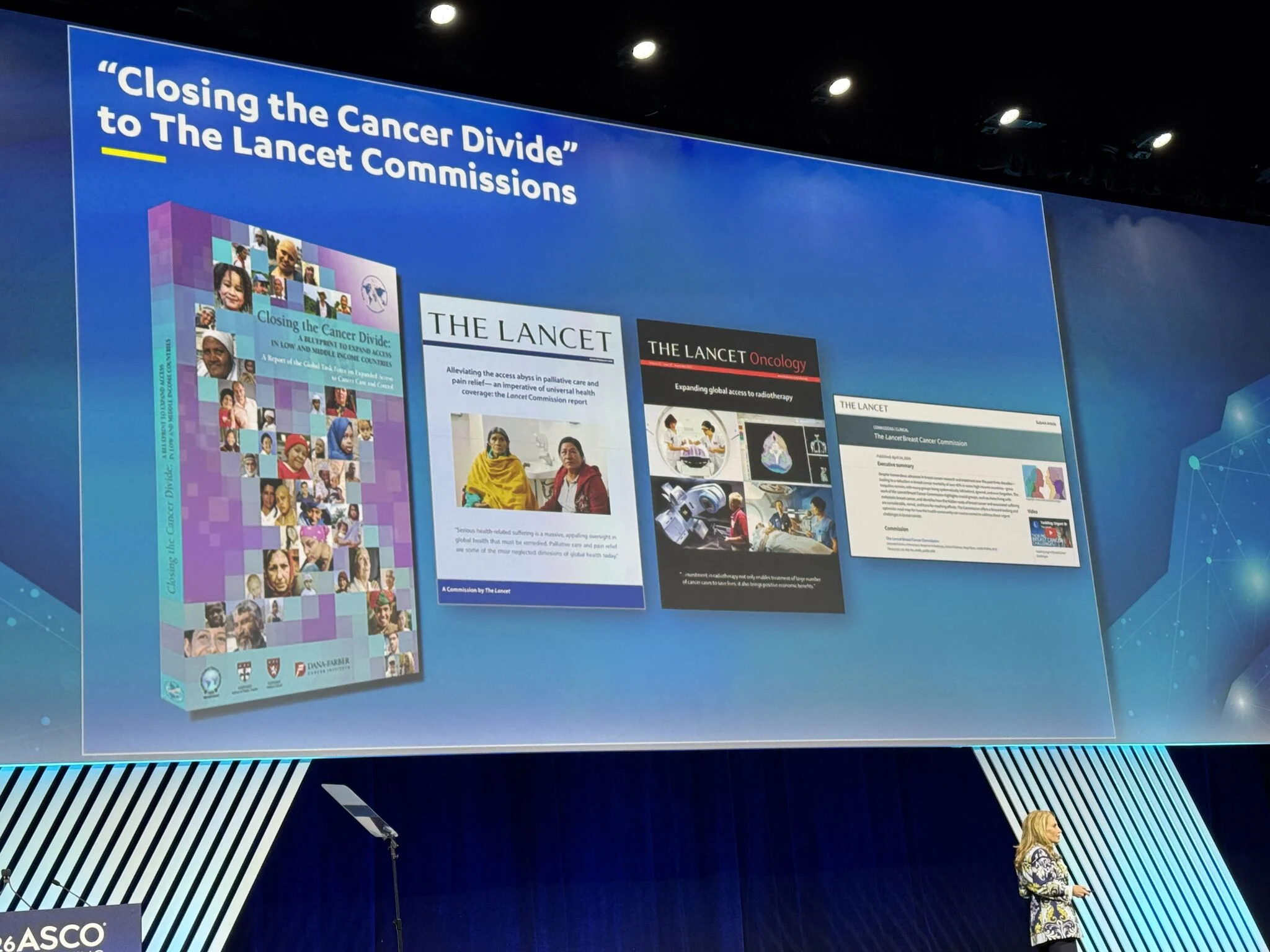
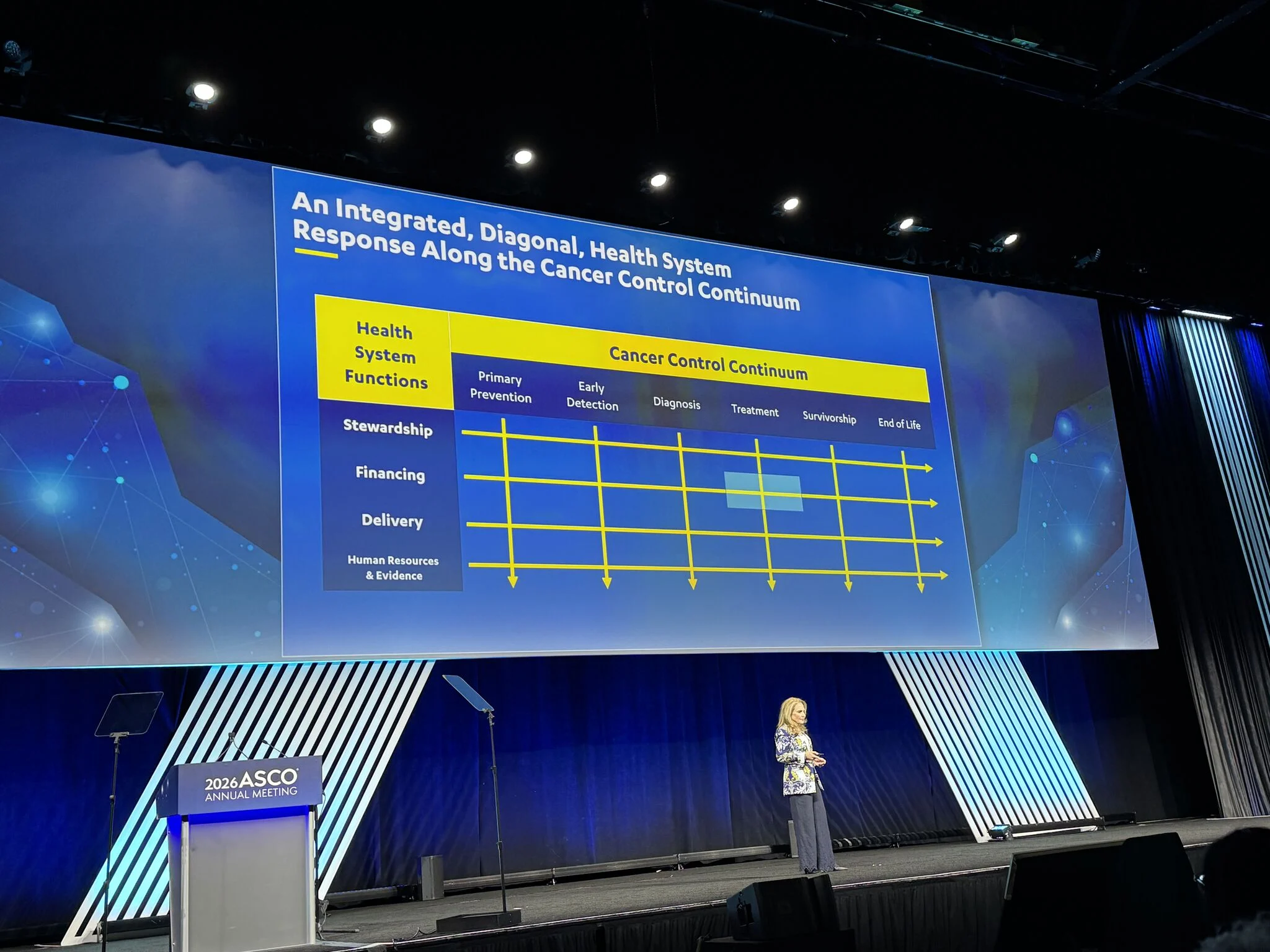
“Powerful duo bridging science and human experience at ASCO26 opening session with Julio Frenk and Felicia Marie Knaul speaking about ՛Cancer As A Driver Of Health Systems: Translating Lived Experience Into Global Lessons՛ ” 
“Important data from ASCO 2026 Poster session
Age alone should not exclude patients from a neoadjuvant strategy in locally advanced colon cancer.
The FOxTROT analysis demonstrates that 6 weeks of pre-operative chemotherapy in elderly and frail patients is feasible, safe, and associated with perioperative outcomes comparable to upfront surgery. Importantly, the findings suggest that older patients may derive particular benefit from a neoadjuvant approach, given the lower likelihood of receiving postoperative chemotherapy.
Another step toward a more individualized, fitness-based approach to colon cancer care.”

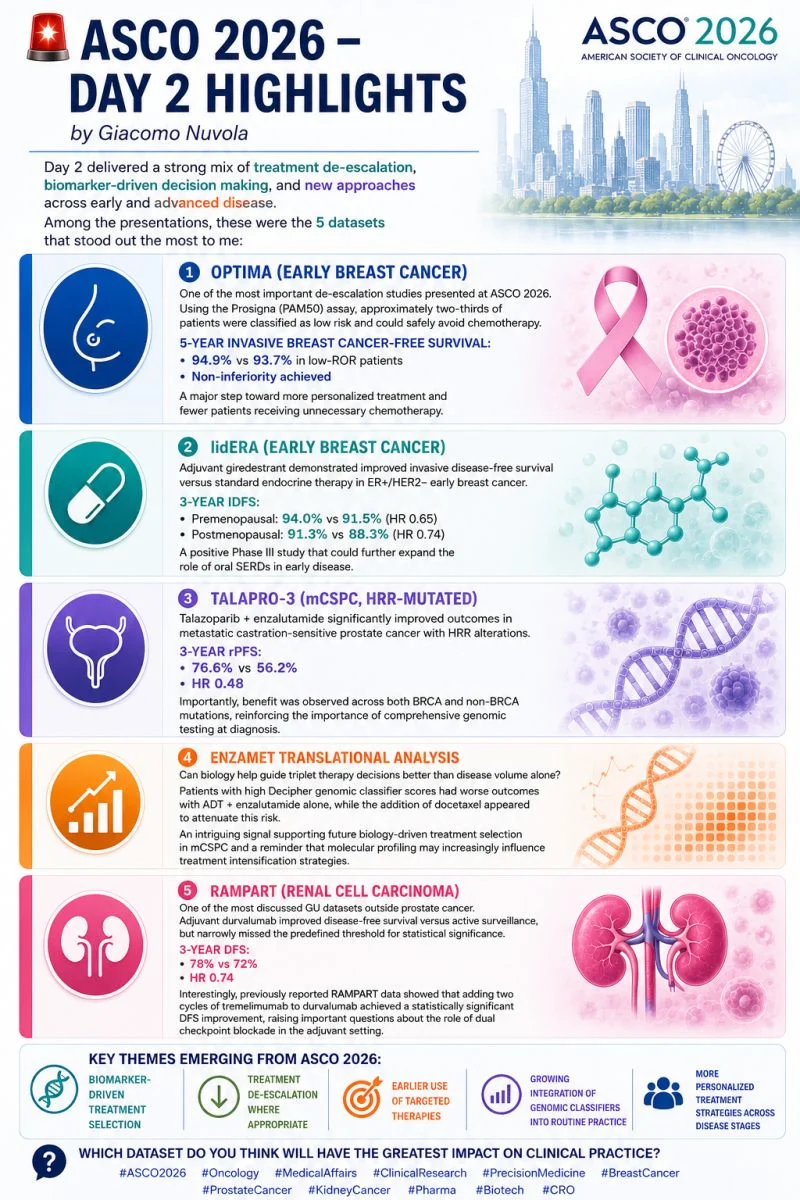
“ASCO 2026 – Day 2 Highlights
Day 2 delivered a strong mix of treatment de-escalation, biomarker-driven decision making, and new approaches across early and advanced disease. Among the presentations, these were the 5 datasets that stood out the most to me:
- OPTIMA (Early Breast Cancer)
One of the most important de-escalation studies presented at ASCO 2026. Using the Prosigna (PAM50) assay, approximately two-thirds of patients were classified as low risk and could safely avoid chemotherapy.
5-year invasive breast cancer-free survival:
- 94.9% vs 93.7% in low-ROR patients
- Non-inferiority achieved
A major step toward more personalized treatment and fewer patients receiving unnecessary chemotherapy.
- lidERA (Early Breast Cancer)
Adjuvant giredestrant demonstrated improved invasive disease-free survival versus standard endocrine therapy in ER+/HER2− early breast cancer.
3-year IDFS:
- Premenopausal: 94.0% vs 91.5% (HR 0.65)
- Postmenopausal: 91.3% vs 88.3% (HR 0.74)
A positive Phase III study that could further expand the role of oral SERDs in early disease.
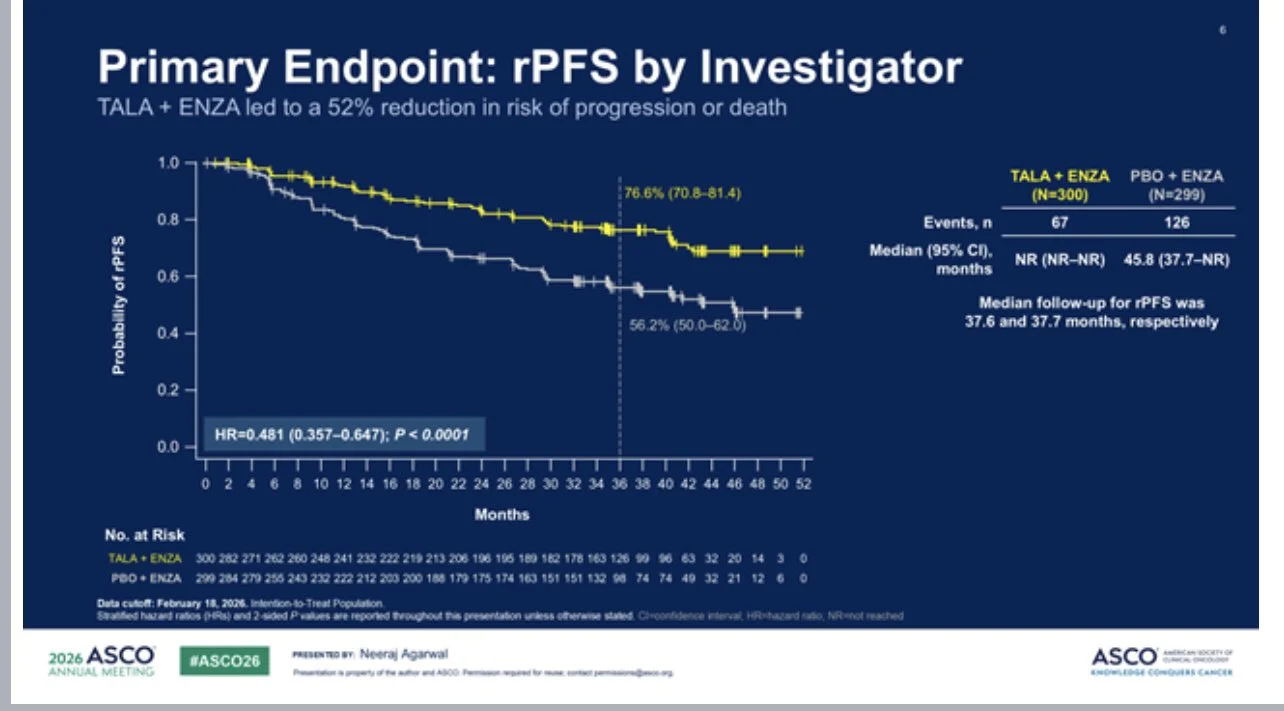
- TALAPRO-3 (mCSPC, HRR-mutated)
Talazoparib + enzalutamide significantly improved outcomes in metastatic castration-sensitive prostate cancer with HRR alterations.
3-year rPFS:
- 76.6% vs 56.2%
- HR 0.48
Importantly, benefit was observed across both BRCA and non-BRCA mutations, reinforcing the importance of comprehensive genomic testing at diagnosis.
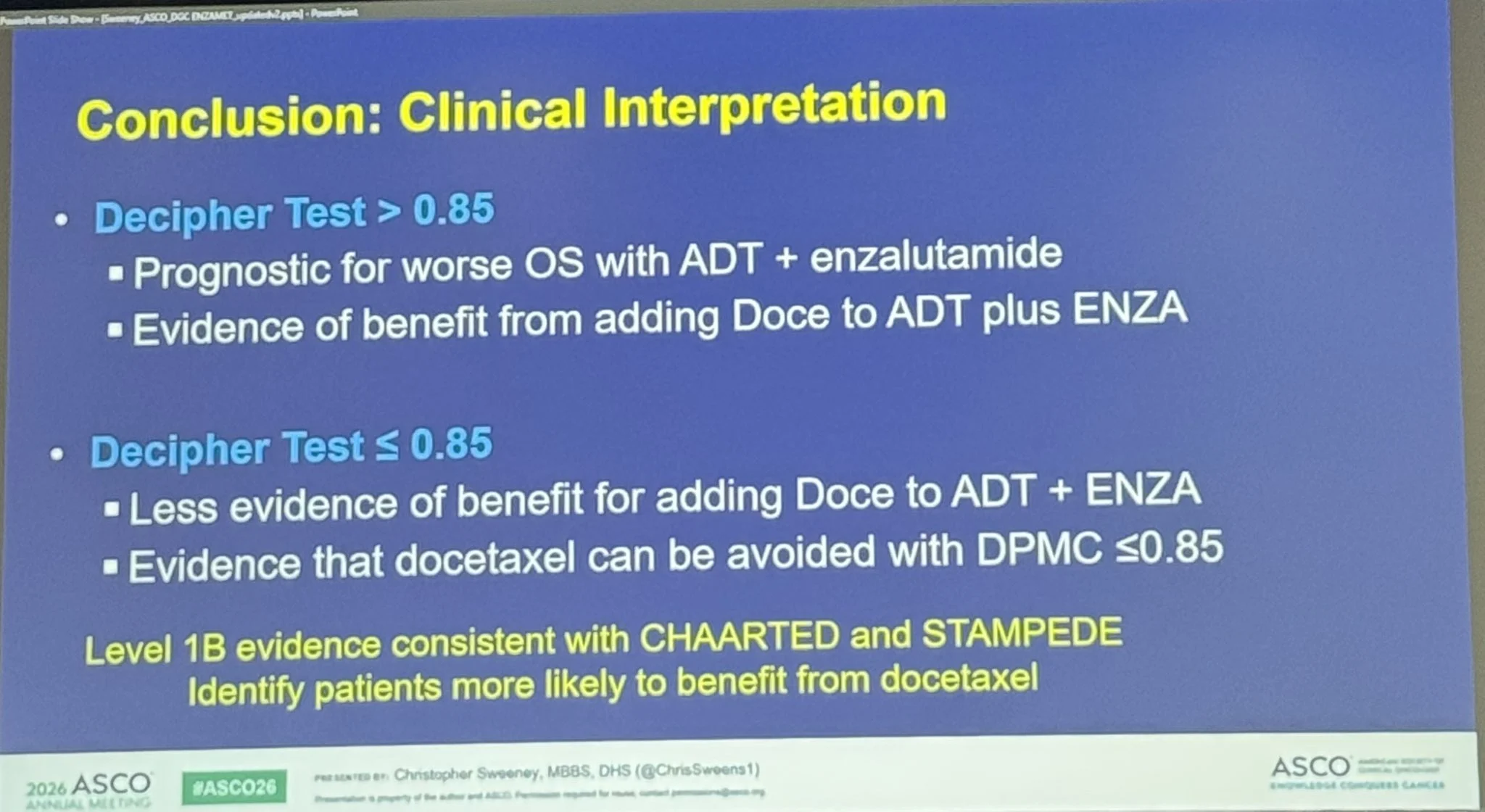
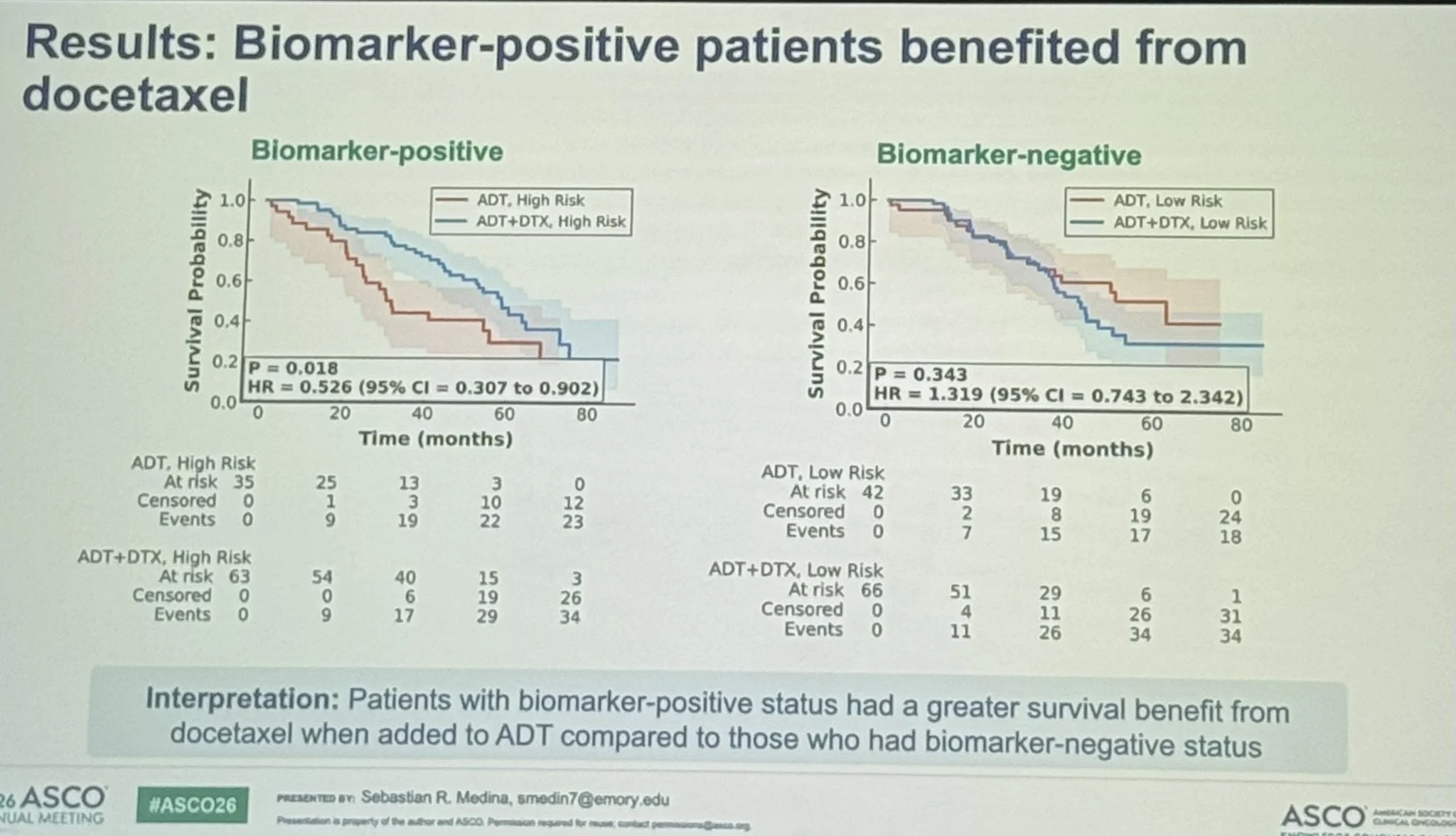
- ENZAMET Translational Analysis
Can biology help guide triplet therapy decisions better than disease volume alone? Patients with high Decipher genomic classifier scores had worse outcomes with ADT + enzalutamide alone, while the addition of docetaxel appeared to attenuate this risk. An intriguing signal supporting future biology-driven treatment selection in mCSPC and a reminder that molecular profiling may increasingly influence treatment intensification strategies.
- RAMPART (Renal Cell Carcinoma)
One of the most discussed GU datasets outside prostate cancer. Adjuvant durvalumab improved disease-free survival versus active surveillance, but narrowly missed the predefined threshold for statistical significance.
3-year DFS:
- 78% vs 72%
- HR 0.74
Interestingly, previously reported RAMPART data showed that adding two cycles of tremelimumab to durvalumab achieved a statistically significant DFS improvement, raising important questions about the role of dual checkpoint blockade in the adjuvant setting.
Key themes emerging from ASCO 2026:
- Biomarker-driven treatment selection
- Treatment de-escalation where appropriate
- Earlier use of targeted therapies
- Growing integration of genomic classifiers into routine practice
- More personalized treatment strategies across disease stages․”
“ASCO26, Breast Cancer Oral Abstract Session – Key Takeaways, 30 May
This year’s breast session converged on a single theme: doing more where it matters, and less where it doesn’t.
A few highlights worth carrying back into clinic
Genomics to de-escalate chemotherapy (OPTIMA, 500)․ In high-clinical-risk ER+/HER2− EBC, a PAM50/Prosigna ROR-directed strategy was non-inferior to standard chemo-endocrine therapy (5-yr IBCFS 90.4% vs 91.5%; HR 0.99). 68% safely avoided chemotherapy – including premenopausal women on OFS and patients with N2 disease. A meaningful step away from anatomy-driven decisions toward biology-driven ones.
Building the CDK4/6i and SERD evidence
- NATALEE gene-expression analysis (501): adjuvant ribociclib benefit was consistent across all PAM50 subtypes (HR 0.42–0.77), with no subtype × treatment interaction.
- lidERA BC (502): adjuvant giredestrant improved IDFS regardless of menopausal status (PRE-M HR 0.65; POST-M HR 0.74), with fewer discontinuations vs AI.
Surgical and local de-escalation
- SENOMAC (LBA503): omitting completion ALND for 1–2 SLN macrometastases was oncologically safe (5-yr OS 94.4% vs 93.4%; HR 0.84) and reduced patient-reported arm morbidity.
- AXSANA (505): in 5,262 cN+ patients, axillary response to NACT was driven by tumor biology, not nodal burden- number of involved nodes at diagnosis did not predict ypN0 (p=0.67). Notably, HR+/HER2− tumors reached nodal pCR in only 31%, questioning the rationale of neoadjuvant chemotherapy aimed at axillary clearance in luminal disease.
- PREPEC/OPBC-02 (504): pre-pectoral reconstruction improved 24-month QoL (+4.8 BREAST-Q points) at the cost of higher implant loss/replacement (21.1% vs 14.5%) – a genuine trade-off to discuss with patients.
Escalation where the risk is real
- KEYNOTE-522 final analysis (507): in high-risk early TNBC, neoadjuvant + adjuvant pembrolizumab maintained its survival benefit at ~7.8 years (7-yr OS 85.1% vs 77.2%; HR 0.64).
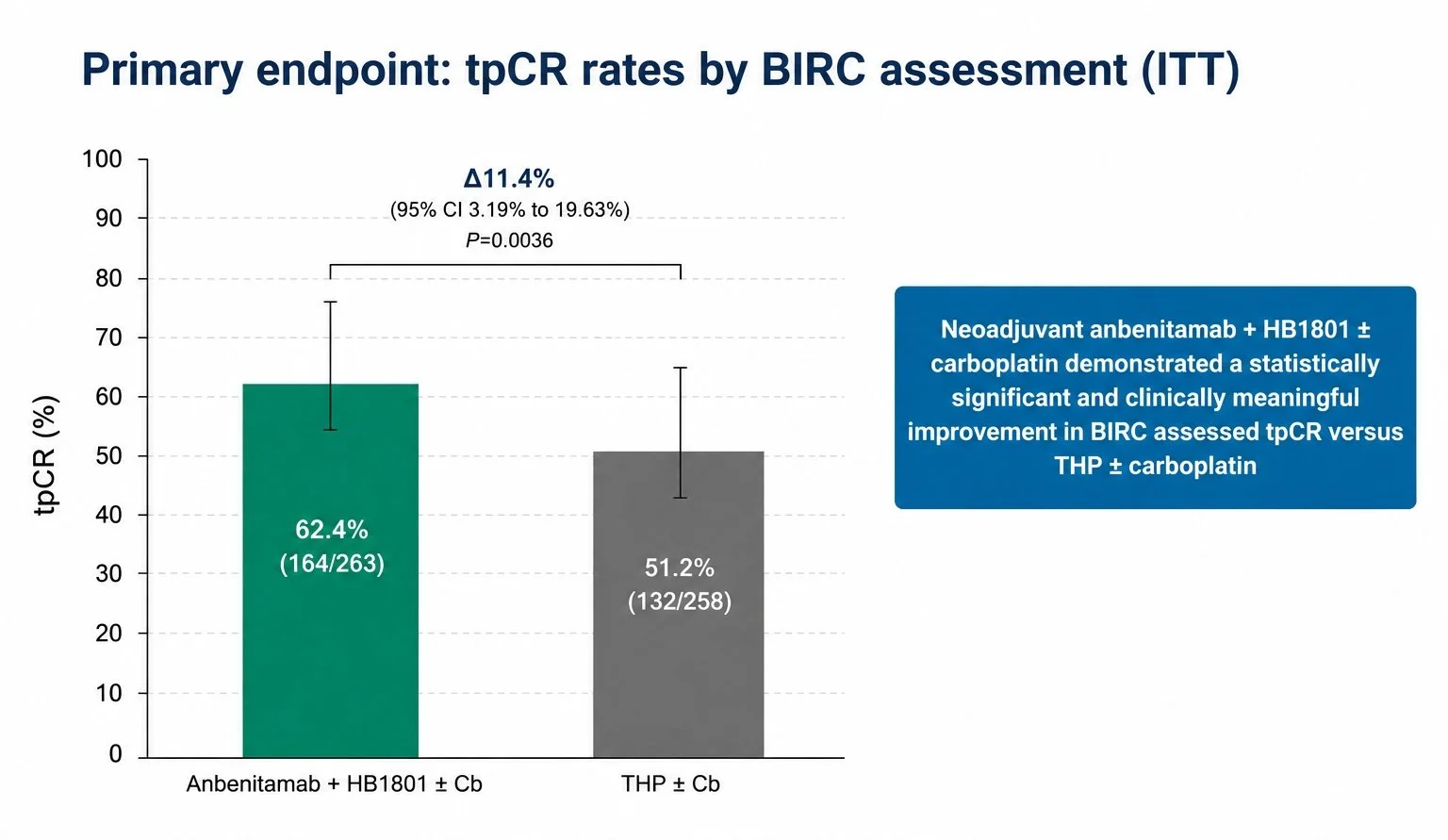
- Anbenitamab (LBA660): the biparatopic anti-HER2 antibody + nab-docetaxel ± Cb improved tpCR vs THP ± Cb (62.4% vs 51.2%). A promising signal – though benchmarked against the previous standard, while T-DXd – THP (DESTINY-Breast11) has now reshaped the neoadjuvant HER2+ landscape.
- A note of caution (506) A small RCT (n=379) of non-cross-resistant adjuvant chemotherapy in HR+/HER2− residual disease reported a 10-yr OS benefit (89.9% vs 82.9%; HR 0.56). Worth flagging that the primary endpoint (DDFS) was only a trend (p=0.059) and OS was a borderline secondary endpoint (p=0.048) with few events – hypothesis-generating, not practice-changing.
Bottom line: the field keeps refining who truly needs intensification and who can be spared it – with biology, not anatomy, increasingly steering the wheel.”

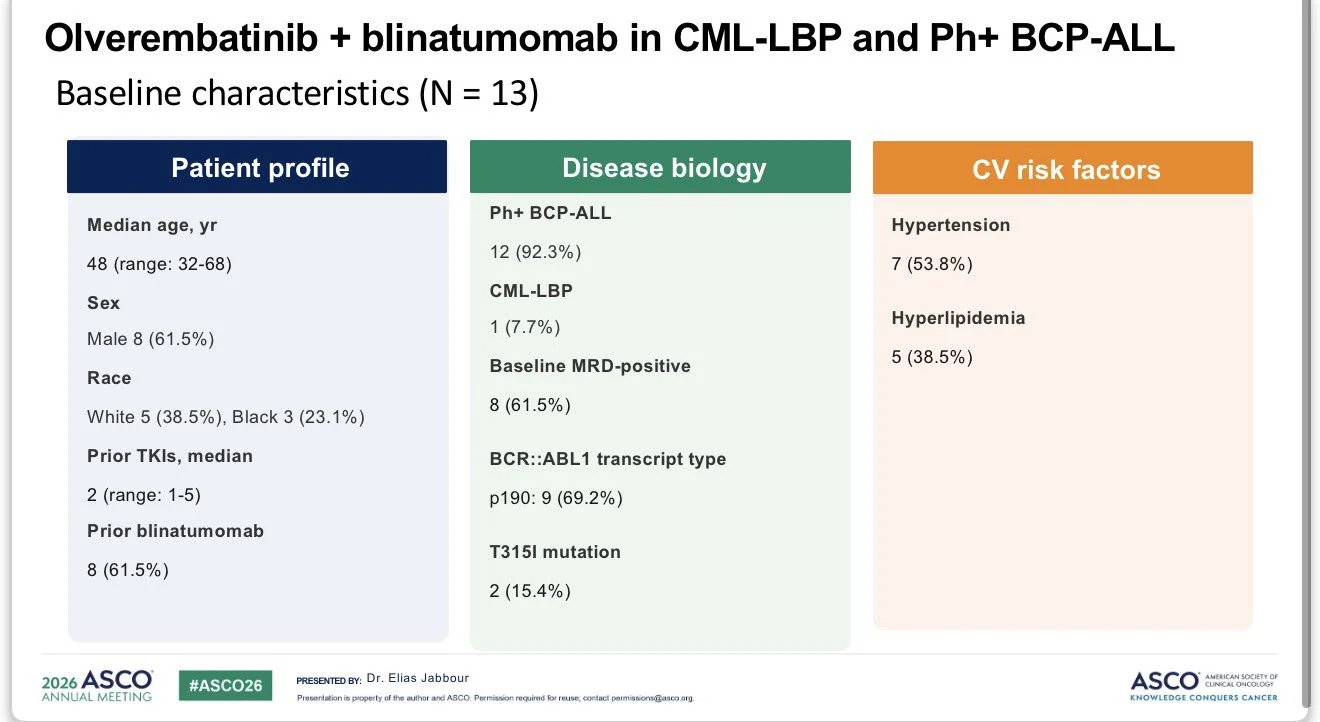
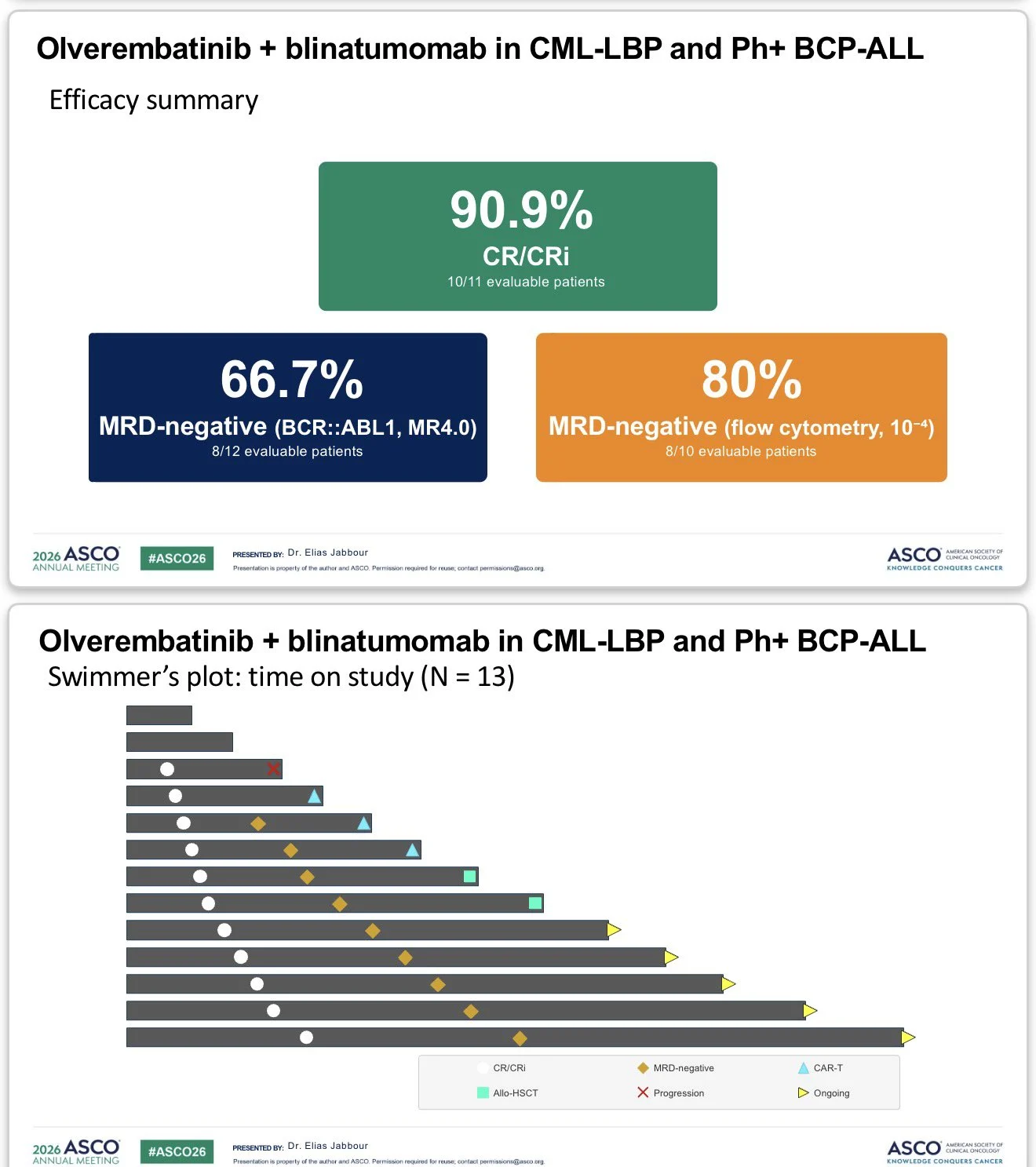
“Chemo-free dual targeting with olverembatinib + blinatumomab shows promising early activity in heavily pretreated Ph+ ALL/CML lymphoid blast phase (n=13):
- CR/CRi: 91% (10/11 evaluable)
- MR4.0: 67%
- Flow MRD−: 80%
- Prior TKIs: median 2 (range 1–5)
- Prior blinatumomab: 62%
- T315I mutation: 15%
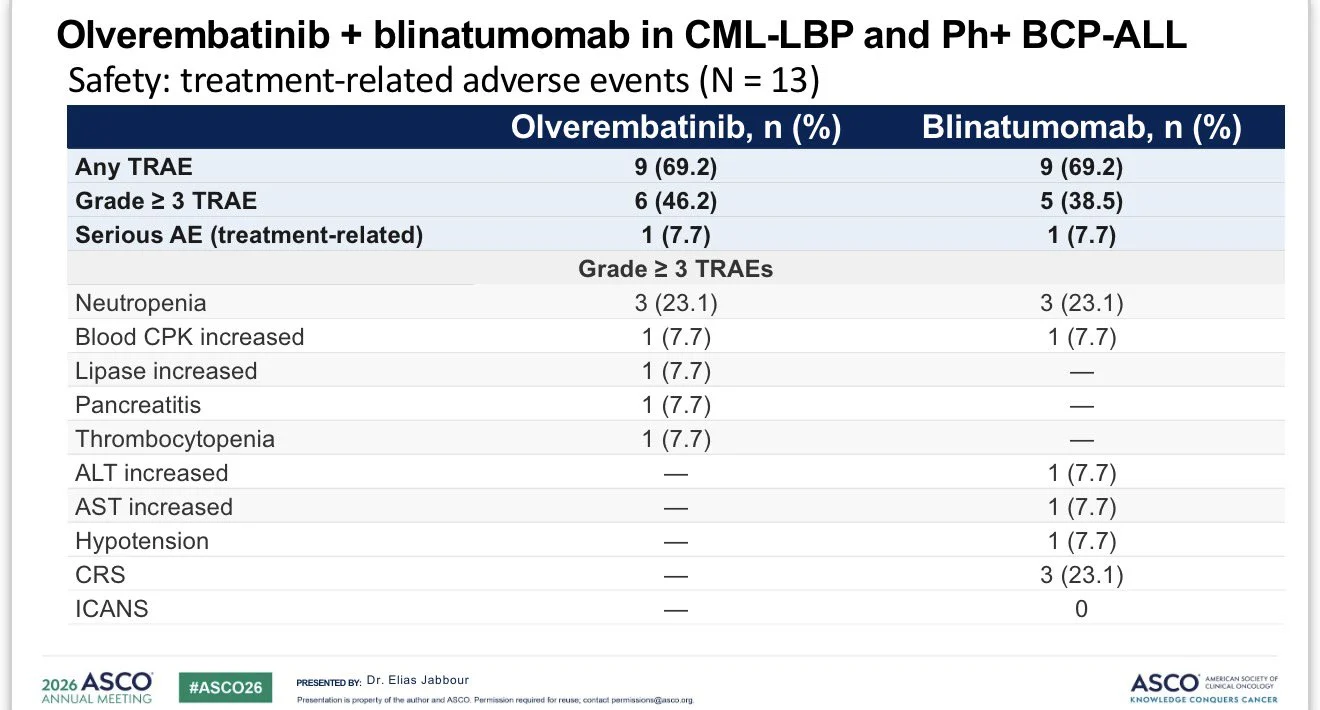
Safety was manageable with low rates of serious toxicity, CRS in 23%, and no ICANS. Early data suggest a potent chemotherapy-free strategy capable of inducing deep remissions even in TKI-resistant disease.”

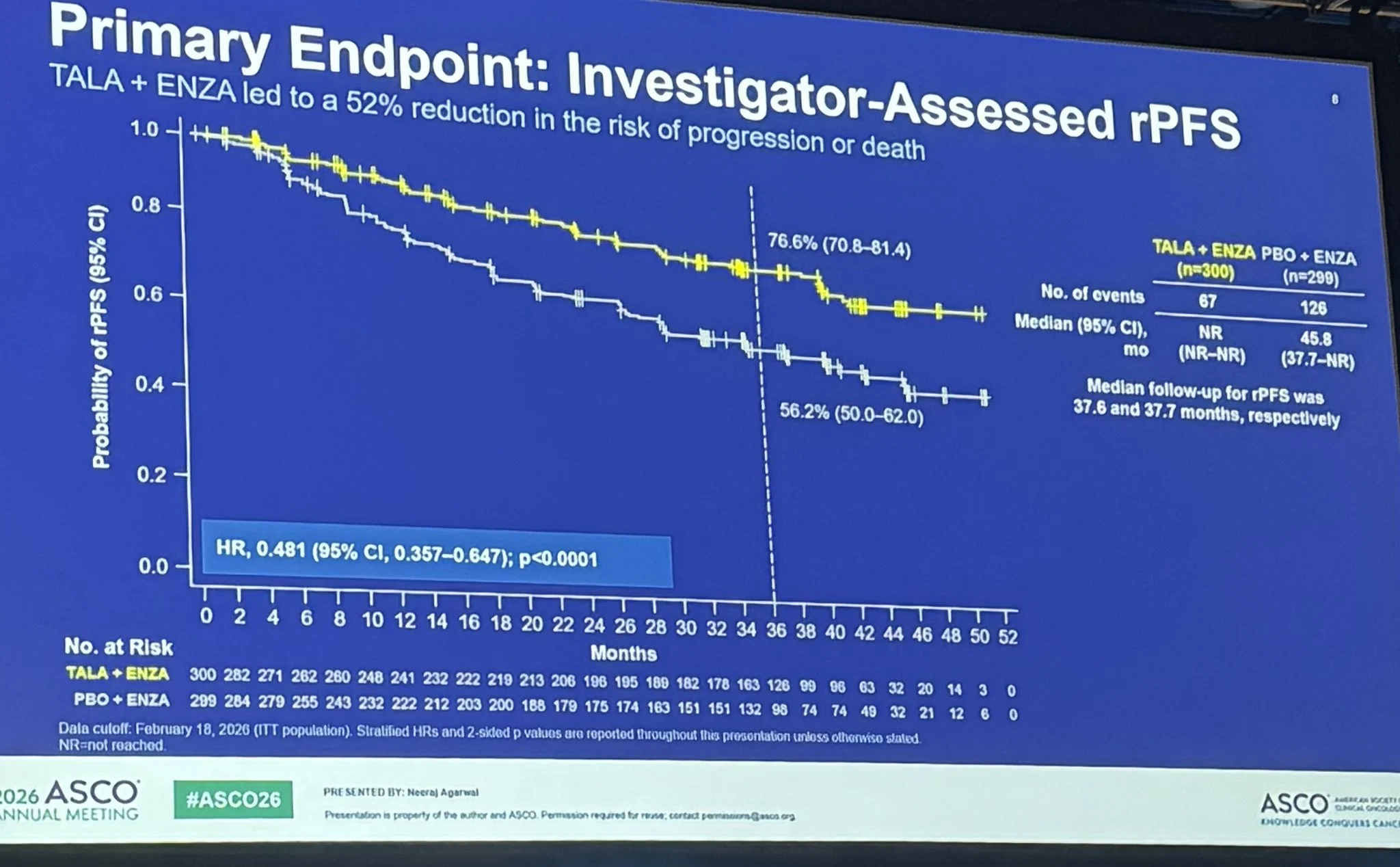
Check Y Axis in both slides. Classic example of length Illusion created to increase visual impact of the difference in two arms. This should be avoided.
What is the difference between Two slides ? One on left is original from ASCO talk. One on right is corrected using AI. This is called as ‘Length illusion’. Common trick to enhance ‘visual’ effect over ‘actual’ effect.”

“Honored to receive the FASCO designation at this year’s ASCO26 opening ceremony.
Amazing to celebrate alongside so many deserving colleagues Komal Jhaveri, Tian Zhang, Emil Lou, Kimmie Ng, Rafeh Naqash, Eleonora Teplinsky and many more also receiving this honor!”

“This is so cool! Not comprehensive…yet, but how amazing that ASCO annual meeting is now going to have live translations. So much more accessible for our colleagues. Even for those who speak good English, for many listening in their native language is easier!”
Jasmine Kamboj added:
“ASCO26 = Inclusive!”
“One of the highlights of 2026 was watching Lindsay Schwartz, receive the American Society of Clinical Oncology (ASCO) Conquer Cancer Career Development Award. This achievement serves as a reminder that the future is bright.”

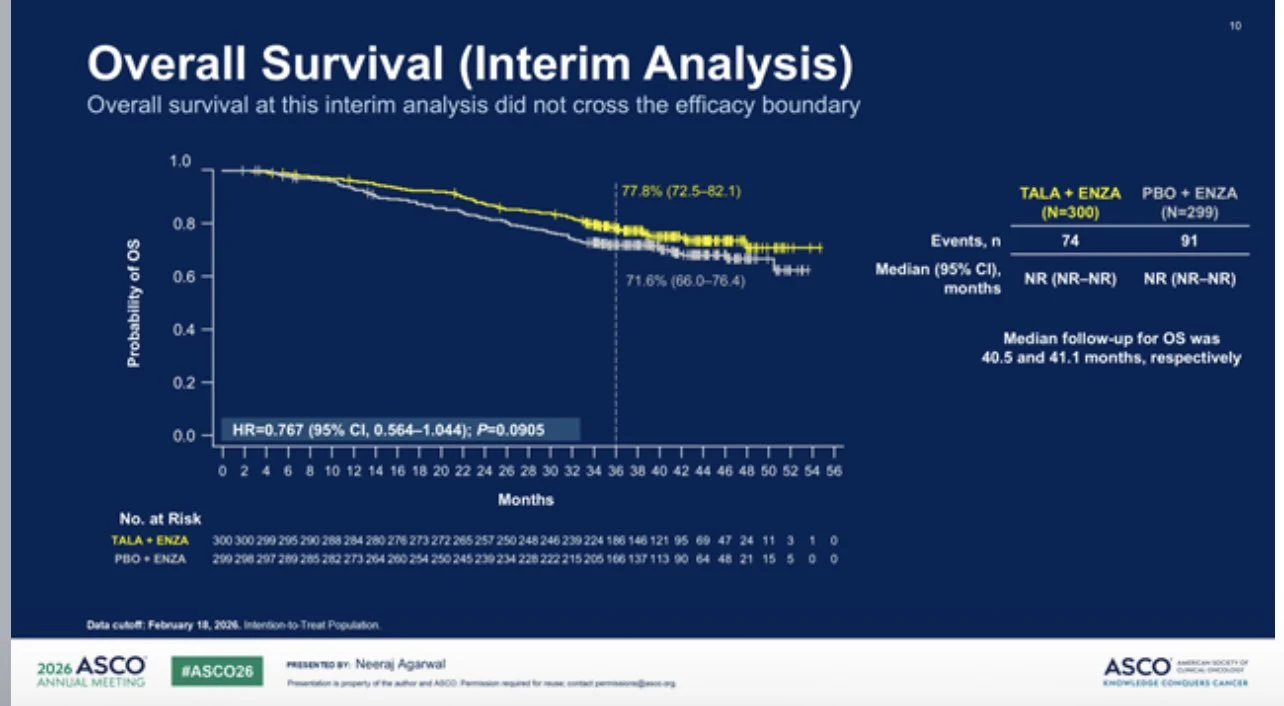
“Big presentation of Day 2 at ASCO26 is TALAPRO3 from Neeraj Agarwal, also published in NEJM.
Phase 3 for ADT/enzalutamide +/- talazoparib for mHSPC with HRR alteration. Primary endpoint met with rPFS (HR 0.48). OS trending favorably but immature. MDS/AML was seen as part of tala toxicity again. Subgroups generally favor adding tala but most notable in BRCA2, ATM, and CDK12.
All metastatic Prostate Cancer patients need genomic testing as part of treatment planning. Adding PARP is reasonable for HRR mutated disease but comes with cumulative toxicity risk. ”

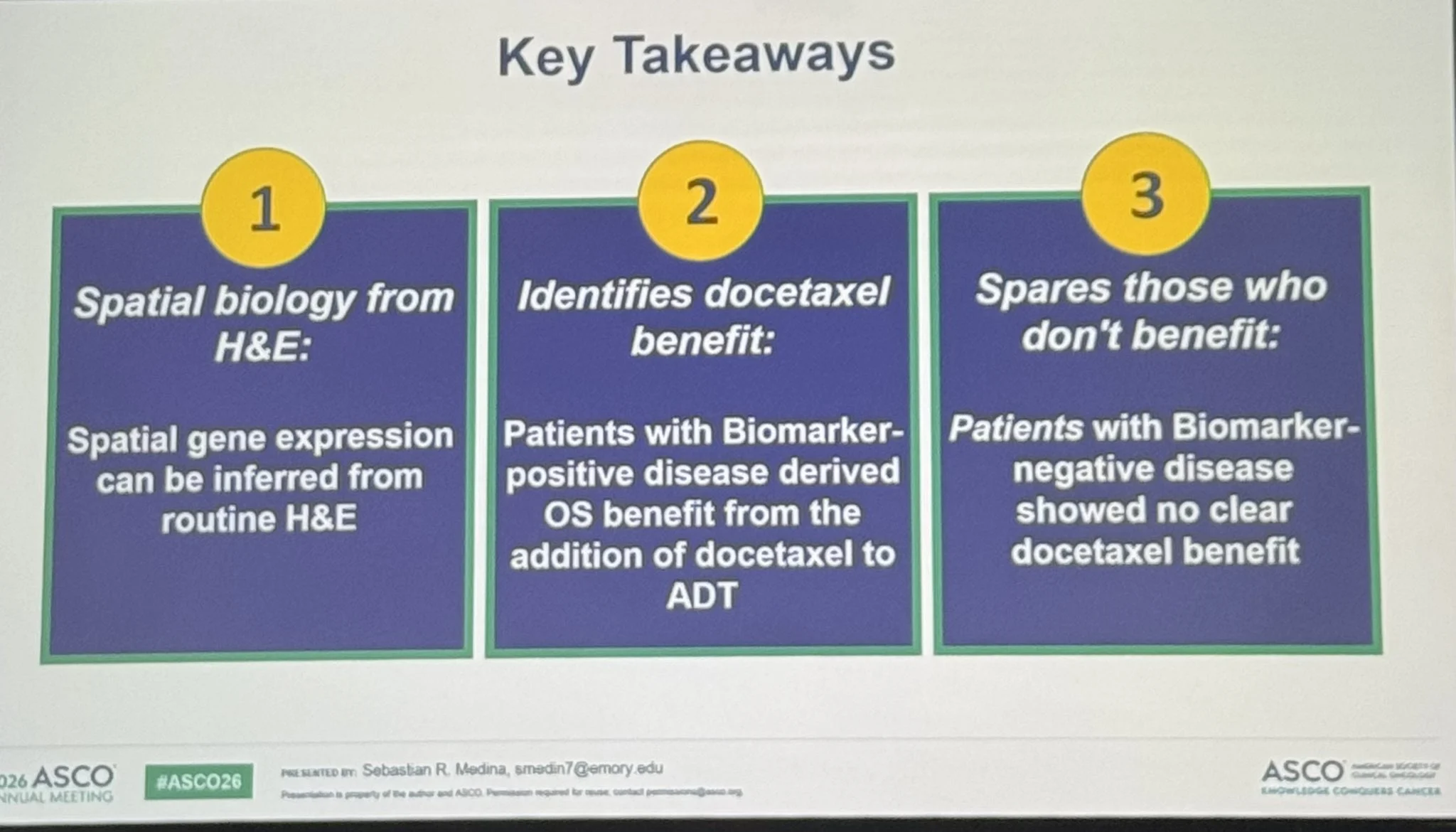
“Two presentations here at ASCO26 focusing on the docetaxel decision for mHSPC.
High decipher (>0.85) suggests docetaxel benefit based on ENZAMET analysis. Novel H&E digital path/spatial transcriptomics AI biomarker using CHAARTED data showed benefit when positive (non-ARPI dataset), no benefit when negative.
We can do better than predicting need for docetaxel based solely on high vs low volume disease, but these are early efforts still. Is clinical assessment based on Gleason, volume, NGS, synchronous vs metachronous disease just as effective?”

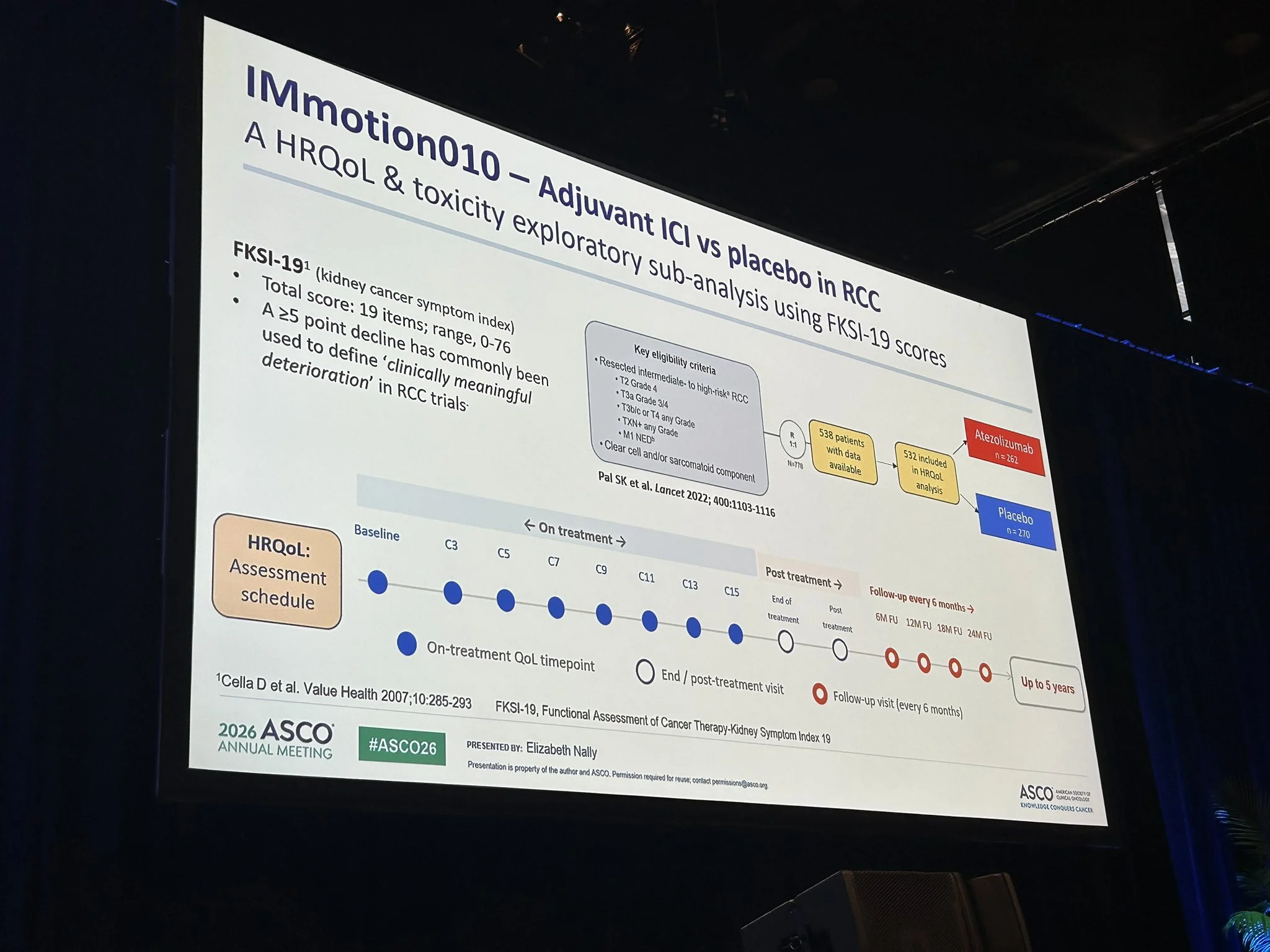
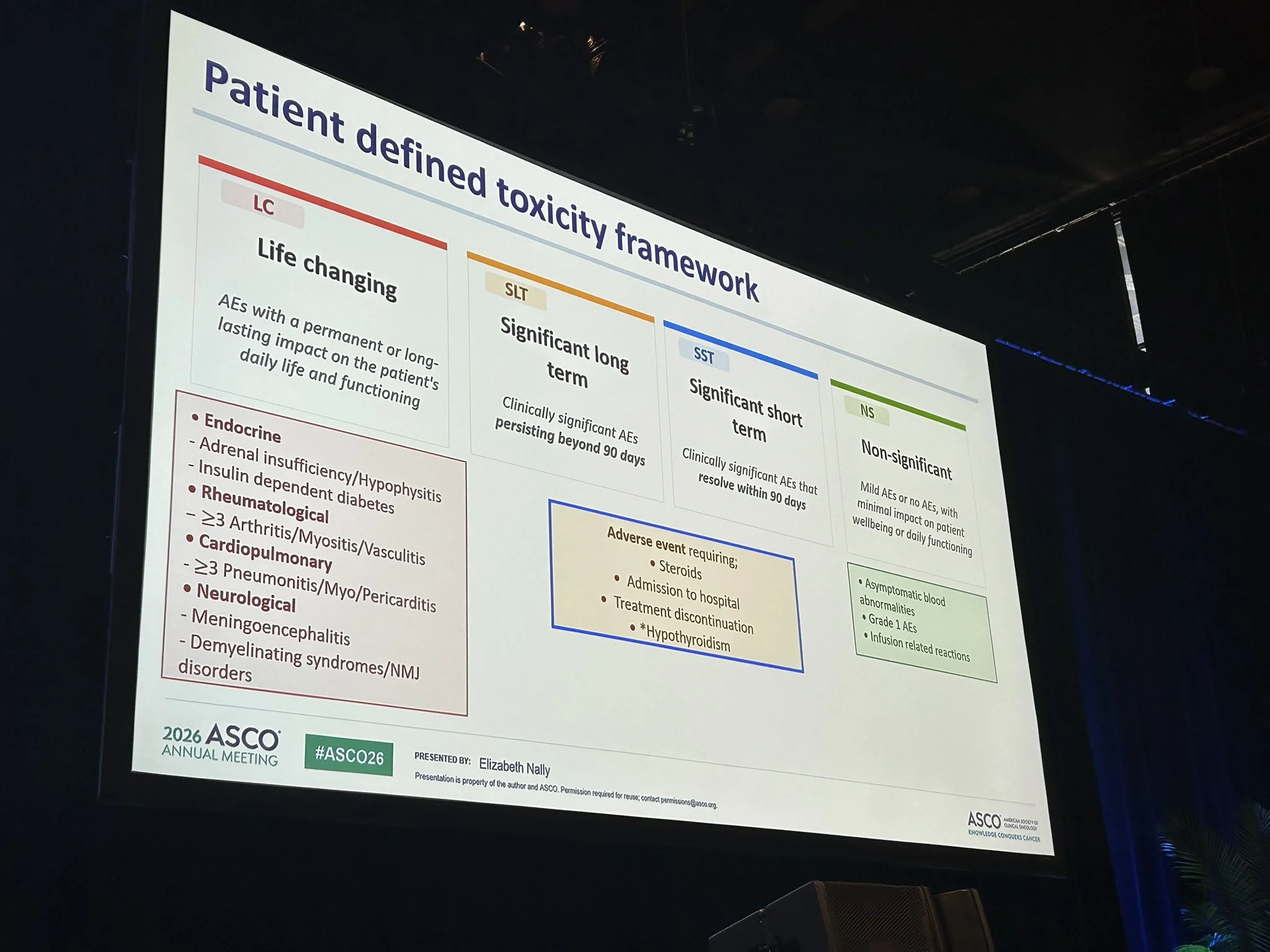
Sumanta K. Pal:
“The best talk I have heard in a long time addressing HRQOL in cancer. With mentorship from Tom Powles, Barts Experimental Cancer Medicine Centre, Beth Nally, presents a pragmatic and meaningful reclassification of toxicity as ‘life-changing’ vs ‘sig long term’ vs ‘sig short term’ vs ‘non-significant’ – definitions arrived at w counsel w patients. From IMmotion010, some phenomenal insights on how this framework could reclassify CTCAE G1-4 tox, a long held frustration in defining the patient experience. Well done!”

”lidERA – ER+/HER2- eBC – showed 3 year iDFS 92.4% with GIRE vs 89.6% SOC ET.
Looked at by menopausal status, premenopausal 41%, post menopausal 59%, pre menopausal iDFS 94% with GIRE vs 91.5% SOC ET, HR 0.65, in post menopausal, 91.3% with GIRE vs 88.3% with SOC ET HR 0.74, improvement also in DFRI in both groups, also fewer pts switched to alternative ET compared to SOC ET and fewer d/c for AE in GIRE vs SOC ET.
Doesn’t appear OFS significantly impacts change in MSK symptoms by way of breakdown by menopausal status.”
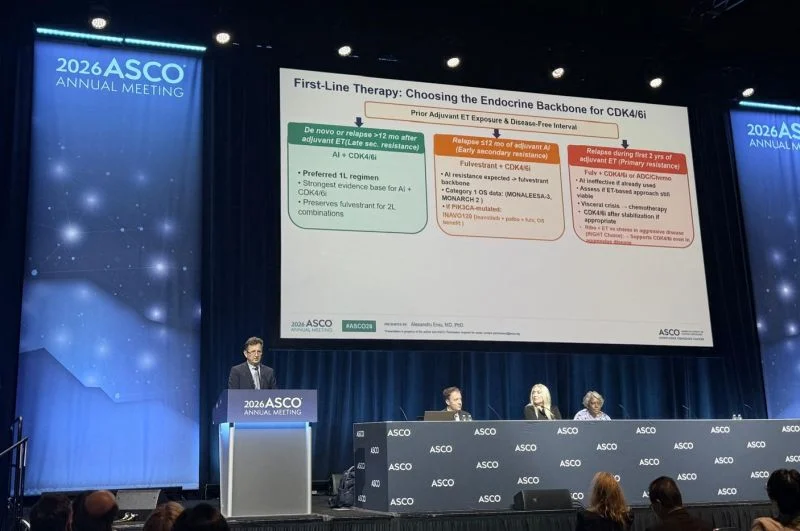
“Chairing and Presenting at ASCO26: Navigating HR+ Metastatic Breast Cancer
Honored to have chaired and presented at the 2026 ASCO Annual Meeting in Chicago yesterday, with a packed Hall D1, a sign of just how pressing this topic is for the oncology community. With 13+ therapeutic options now available for HR+/HER2- metastatic breast cancer, the challenge is no longer ‘what can we give?’ but ‘in what order, and for whom?’
The reality is: we don’t have randomized data for every possible therapeutic sequence. Algorithms alone can’t cover every clinical scenario.
That’s why I proposed a Decision Framework, beyond the algorithm, built on 5 integrated dimensions:
- Biology: What does the tumor tell us? (ER/PR/HER2, ESR1, PIK3CA/AKT1/PTEN, BRCA1/2, tumor-agnostic markers)
- Disease Kinetics: How fast is this moving? (tempo of progression, visceral crisis, disease burden)
- Prior Therapies: What was the tumor exposed to? (duration of benefit, lines of ET, primary vs. secondary resistance)
- Patient: What matters to this person? (age, frailty, comorbidities, QoL priorities, goals of care)
- Logistics and Access: What is actually feasible? (drug availability, cost, global disparities, trial access)
When guidelines are offering several options, a structured framework helps us make individualized, evidence-informed decisions.
Grateful to ASCO for the opportunity and to all the colleagues who joined the discussion.”

“CROWN (5-yr) – Lorlatinib vs crizotinib:
- PFS not reached vs 9.1 mo
- 5-yr PFS: 60% vs 8%
- HR 0.19, Amazing result
Unprecedented durability in ALK+ NSCLC.”

“This morning at ASCO26, NCI Director Dr. Anthony Letai delivered opening session remarks focused on stability, transparency, and the future of cancer research.
Dr. Letai addressed key questions surrounding the FY26 funding environment, including grant timelines, evolving funding strategies, multi-year funding approaches, and support for the extramural research community and early-stage investigators.
‘Our commitment to advancing cancer research has not faltered,’ Dr. Letai shared. ‘The mission has not changed, and the resources to pursue that mission remain in place.’
He also highlighted several areas where NCI is focused on accelerating progress for patients, including:
- Improving clinical trial speed and efficiency
- Functional precision medicine
- Responsible AI integration in the clinical trials ecosystem
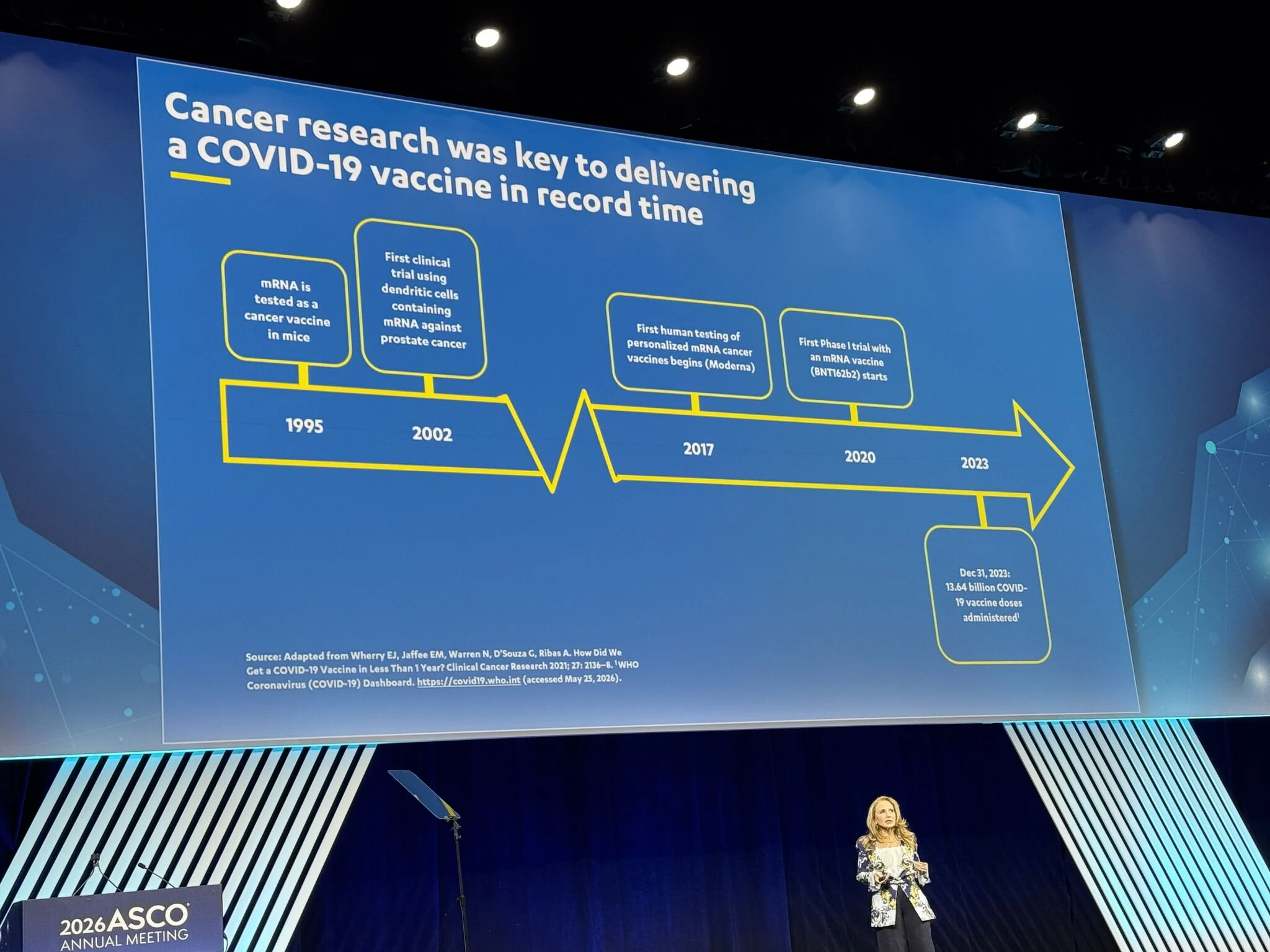
- Cancer therapeutic vaccines
- Prevention, screening, and early detection initiatives
A central theme throughout the remarks was the importance of reducing friction across the research ecosystem while maintaining transparency and accountability for the oncology community.
Thank you to everyone who attended and contributed to the important conversations shaping the future of cancer care and research at ASCO26.”

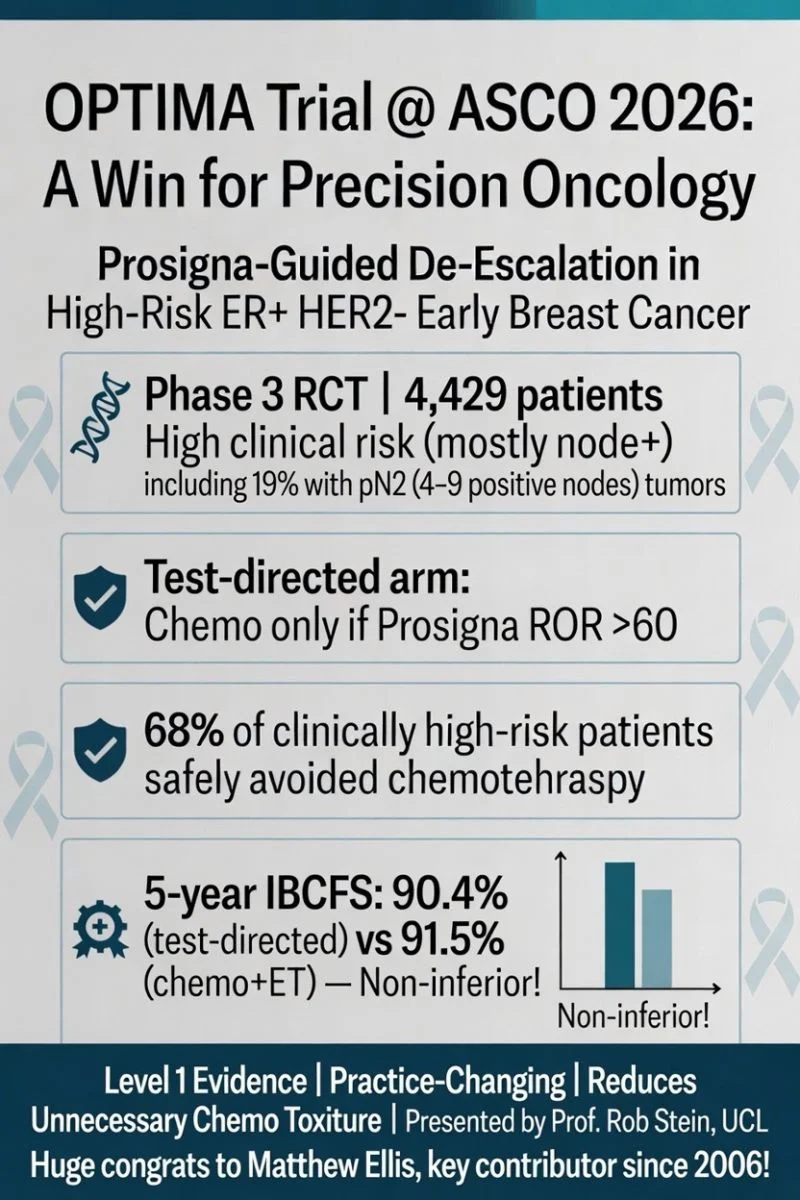
“Landmark OPTIMA trial results presented today at ASCO2026!
Prosigna-guided treatment is non-inferior to chemo + endocrine therapy in high clinical risk ER+ HER2- early breast cancer – including 19% with pN2 (4–9 node+) disease.
~68% of clinically high-risk node-positive patients with low ROR safely avoided chemotherapy while maintaining excellent outcomes.
Level 1 evidence that changes practice and reduces unnecessary toxicity. Huge congrats to my friend Matthew Ellis, key contributor since 2006!”
“Though I want to see more follow-up, this trial is practice changing.
For the first time we see almost no chemotherapy benefit in ROR low risk premenopausal patients who all received ovarian suppression! Supports other ongoing trials like OFSET!”
“A little oxytocin boost during a busy ASCO.
Being a physician scientist and a healer is incredible, and it can also be draining. It helps to recharge with people who understand both the excitement and the challenges.
Thank you to Debbie’s Dream Foundation and Amanda for bringing us together, highlighting our stories, and of course documenting the fabulous ASCO26 fashion with this photo. Now back to work.”

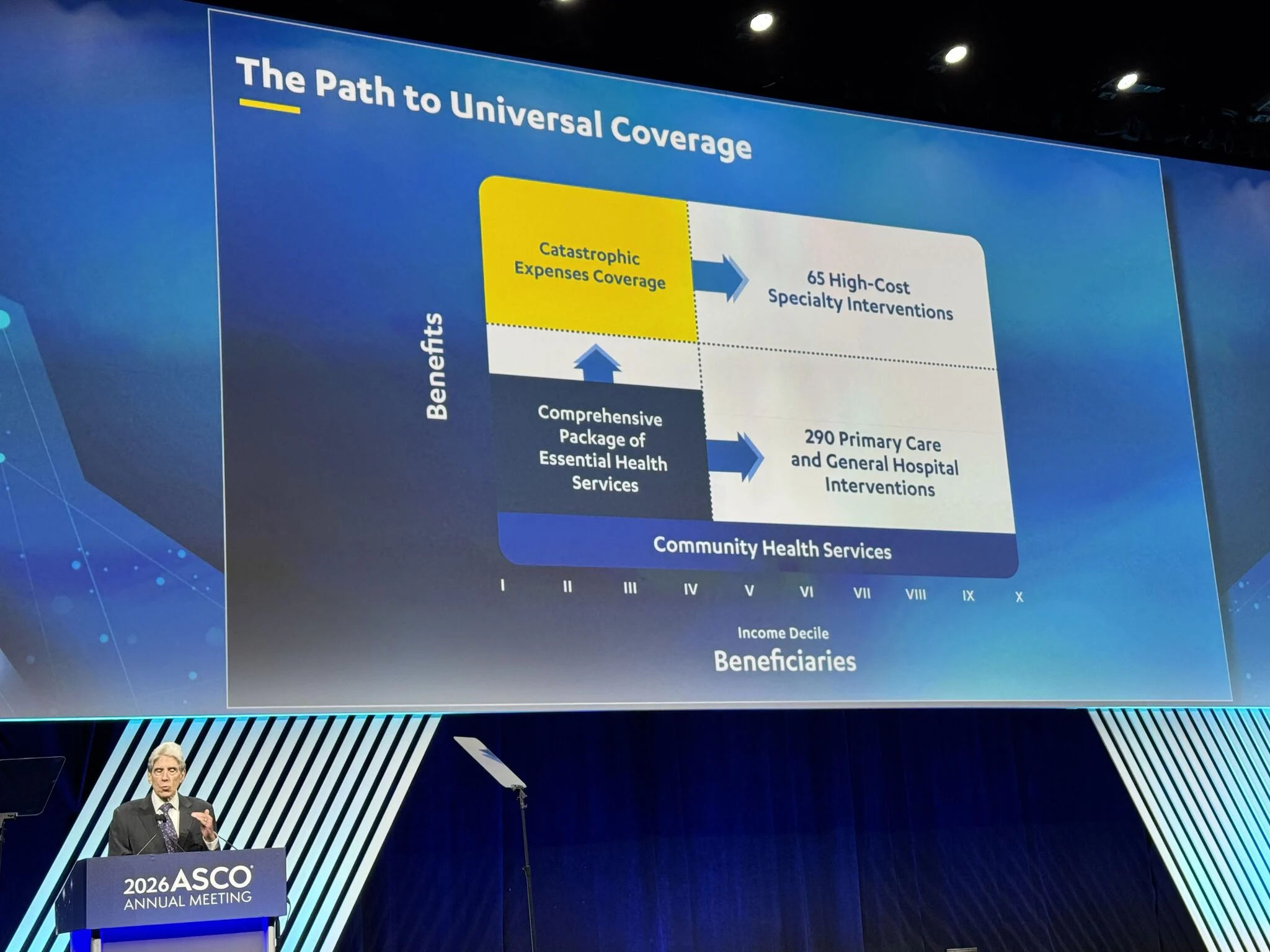
“Value, Access and Quality Care: Can We Have It All?
Some hard conversations ahead as health systems make judgements about value in care amid rising financial costs and constrained budgets. However, it is possible to work together on solutions.
Thanks Ian, Brooke, Haydeé Verduzco and Ajay Aggarwal for showing us the challenges and opportunities, if we choose to take them on.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}