


The ESMO Congress 2025 is a major global oncology event organized by the European Society for Medical Oncology (ESMO). It is taking place at Messe Berlin in Berlin, Germany from October 17 to 21, 2025. The congress features a comprehensive scientific and educational program designed to foster exchange and debate in translational cancer science, showcasing potentially practice-changing data, and stimulating multidisciplinary discussions to improve cancer treatment options.
Amol Akhade, Senior Consultant at Fortis Hospitals Mumbai, shared highlights from ESMO25 on X:
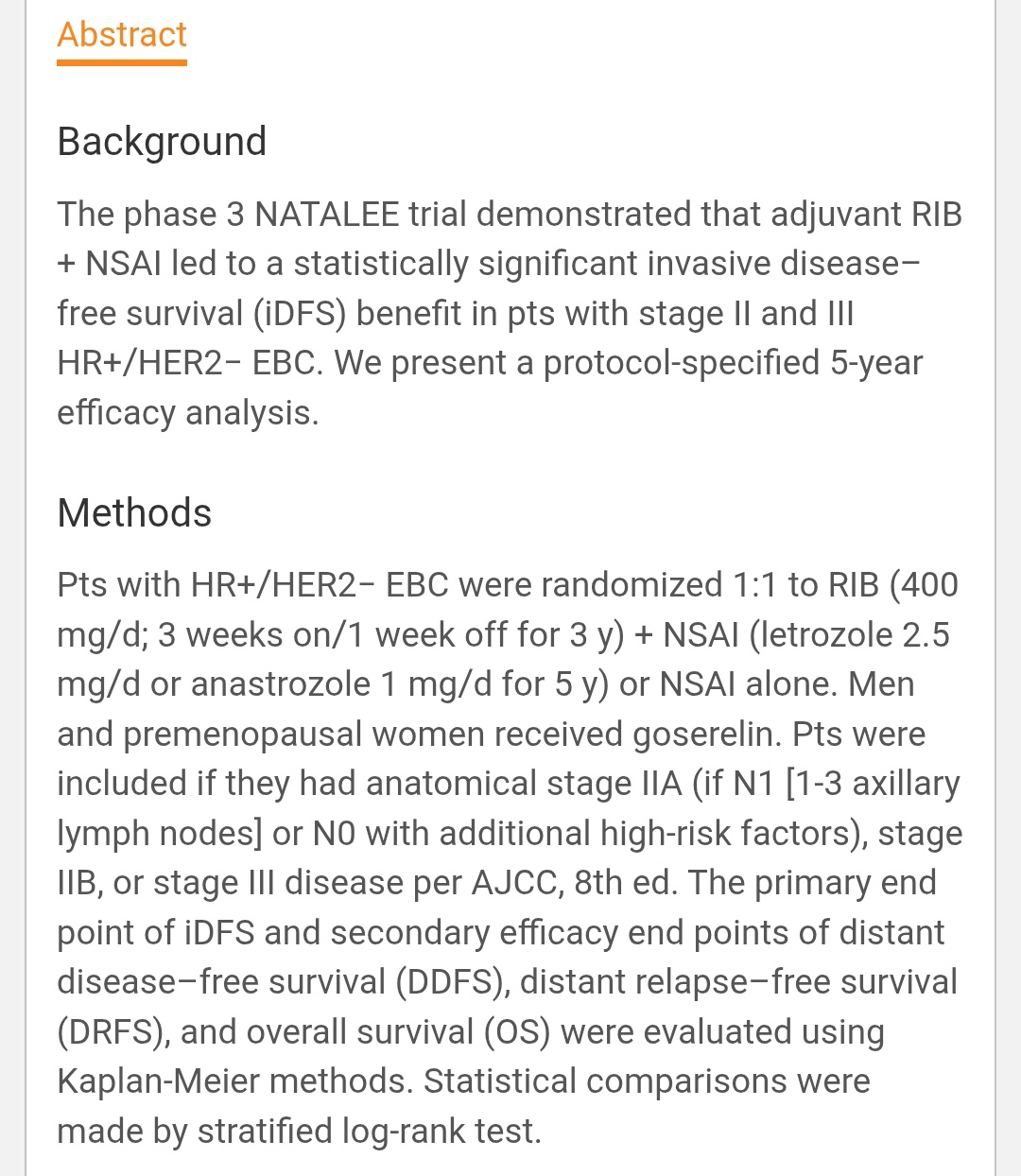
“ESMO 2025 | LBA14 – NATALEE 5-Year Update
Adjuvant Ribociclib (RIB) + NSAI in HR+/HER2– Early Breast Cancer
Longer follow-up, same direction – benefit sustained beyond treatment period.
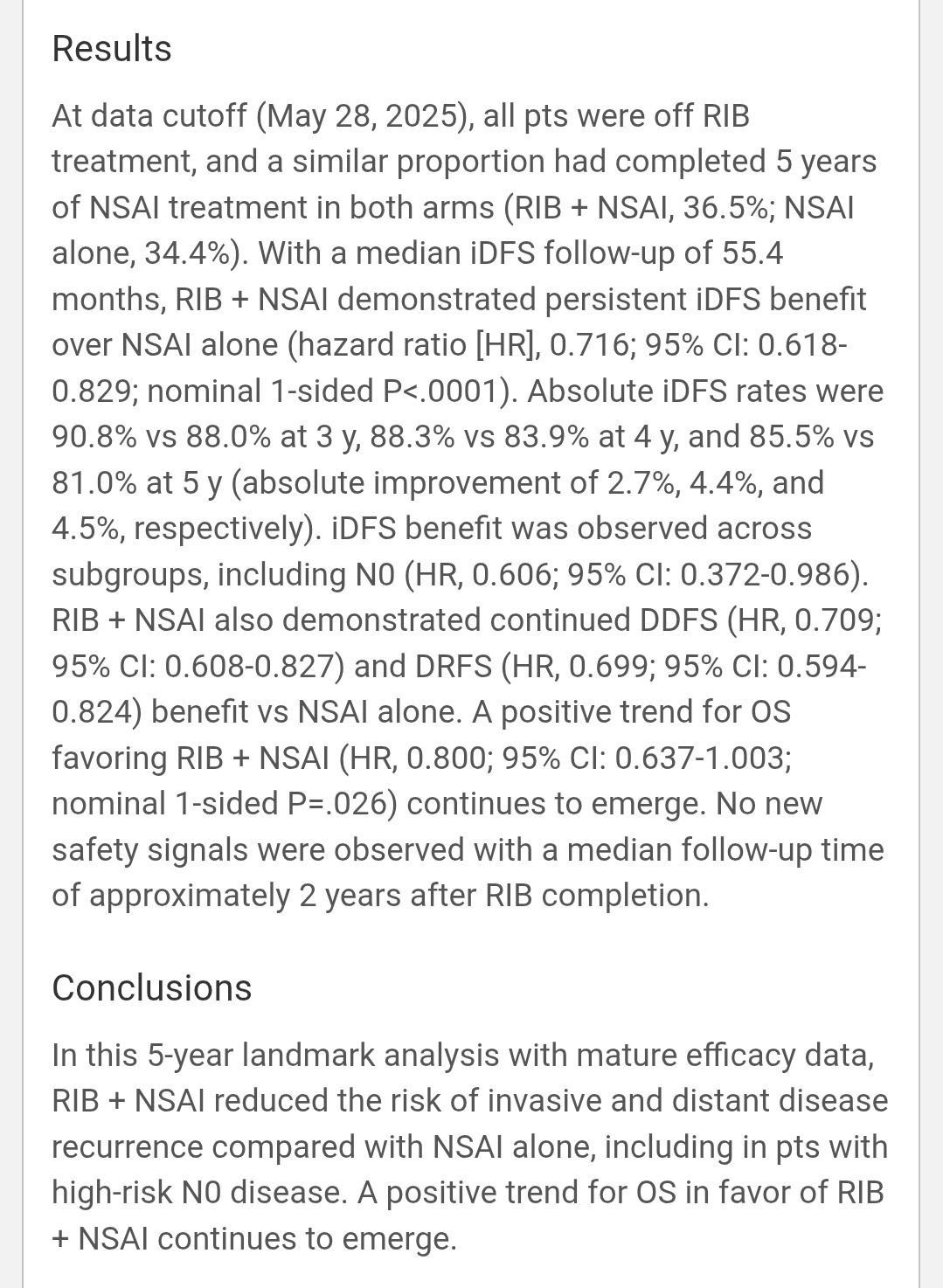
Key Results (median follow-up 55.4 mo)
iDFS HR 0.716 (95% CI 0.618–0.829; p < 0.0001)
Absolute iDFS:
• 3 y 90.8 vs 88.0 % (+2.7)
• 4 y 88.3 vs 83.9 % (+4.4)
• 5 y 85.5 vs 81.0 % (+4.5) DDFS HR 0.709,
DRFS HR 0.699
OS HR 0.80 (95% CI 0.64–1.00) – trend emerging.
Benefit consistent across subgroups, incl. high-risk N0 (HR 0.606).
No new late safety signals 2 y after completion.
OS benefit not yet significant but trending favorably.”

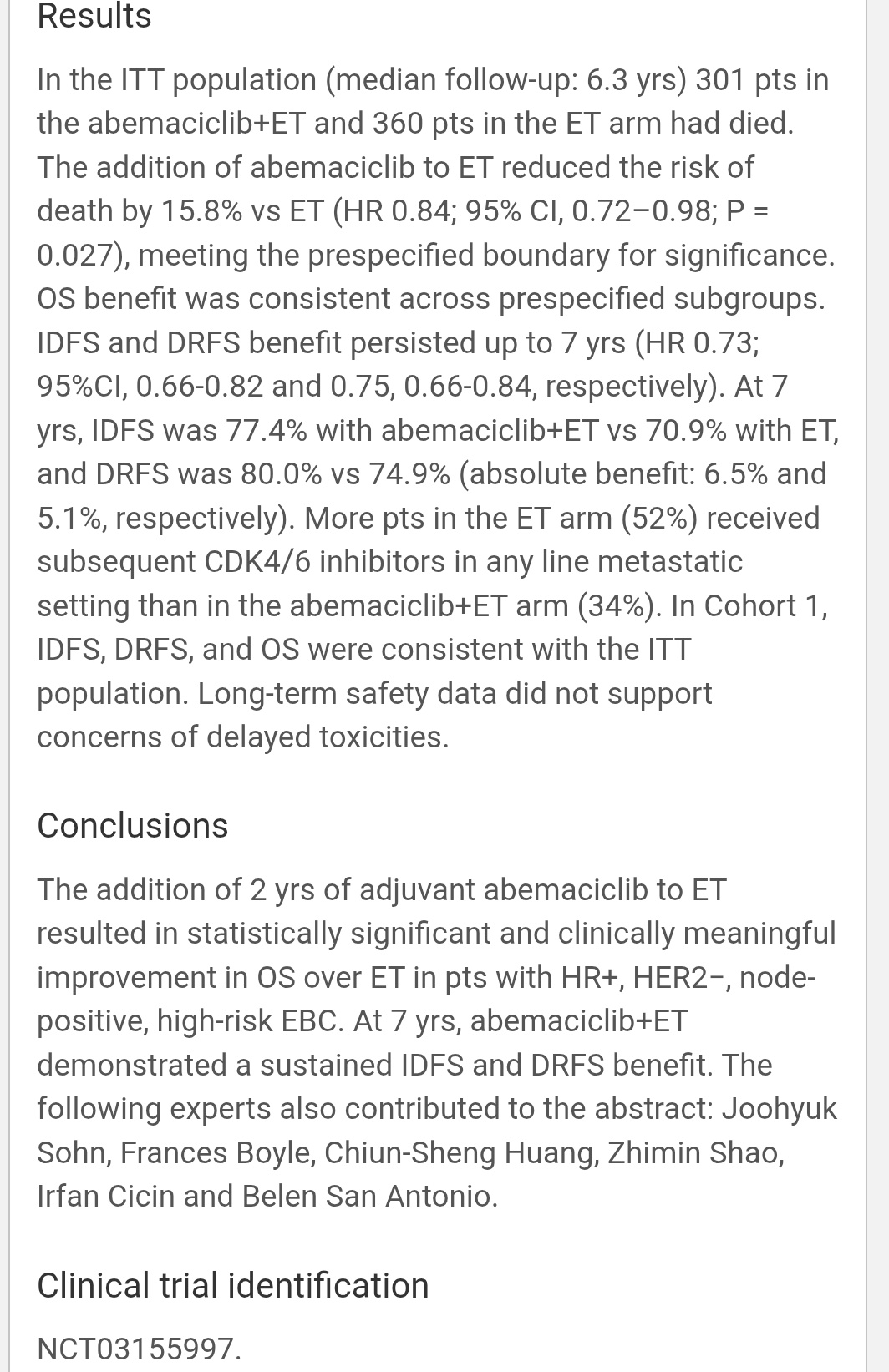
“For HR+, HER2–, node+ high-risk EBC, 2 years of adjuvant abemaciclib + ET showed:
- OS benefit: ↓ risk of death by 15.8% (HR 0.84, p = 0.027)
- 7-yr IDFS: 77.4 vs 70.9% (+6.5%)
- 7-yr DRFS: 80 vs 74.9% (+5.1%)
Benefit consistent across subgroups, durable beyond therapy end, despite crossover (52% ET-alone later got CDK4/6i). Conclusion – First CDK4/6i to show OS gain in early HR+ breast cancer. Abemaciclib now cements its place as standard of care for high-risk adjuvant setting.”

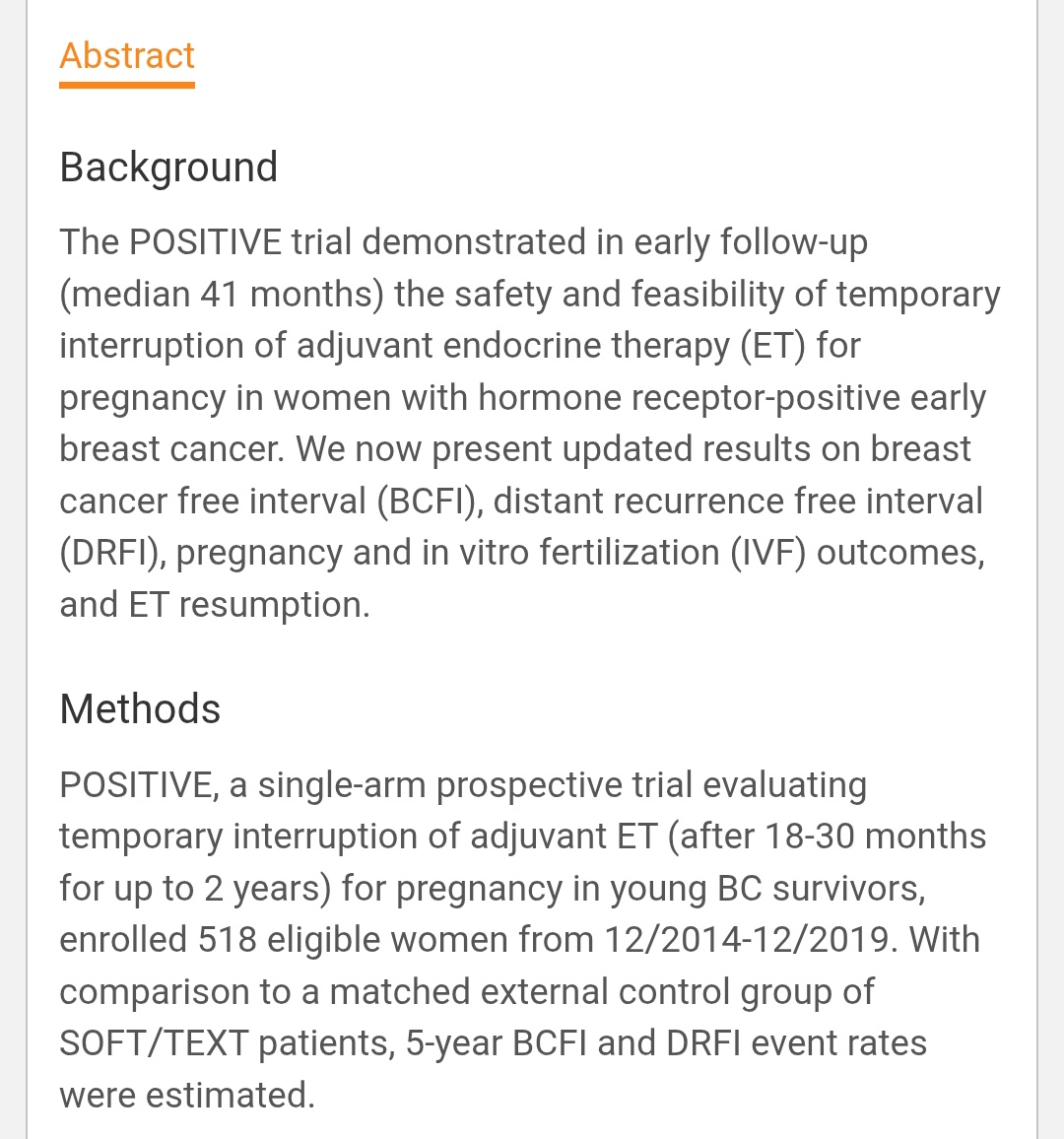
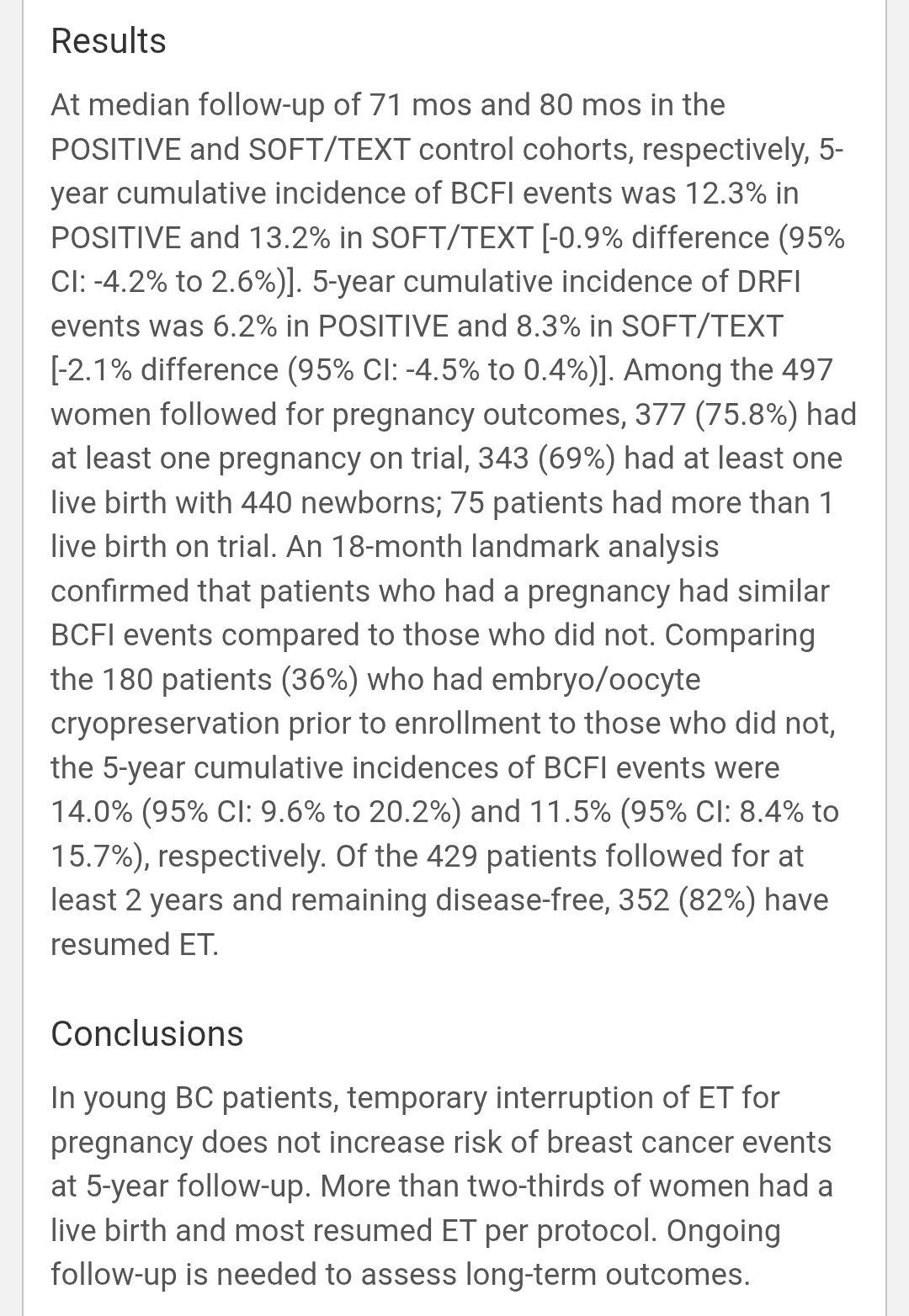
“POSITIVE trial (ESMO 2025, LBA12)
5-year follow-up confirms it’s safe to pause endocrine therapy for pregnancy in young HR+ early breast cancer survivors.
Key findings:
• 518 women, median f/u 71 mo
• 5-yr BCFI: 12.3% vs 13.2% (SOFT/TEXT)
• 5-yr DRFI: 6.2% vs 8.3%
• 76% conceived, 69% had ≥1 live birth (440 babies!)
• 82% resumed ET after ≥2 yrs disease-free
Takeaway: Temporary ET interruption for pregnancy ≠ higher recurrence risk at 5 yrs.
Safe, feasible & empowering.”

“ESMO 2025 | LBA92 ARASAFE
Triplet therapy in mHSPC redefined?
ADT + Darolutamide + Docetaxel D75 = 75 mg/m² Q3W (ARASENS) D50 = 50 mg/m² Q2W
Results:
Grade 3-5 AEs: 61.2% vs 78.9% (p = 0.0024)
NAER (G3/4 neutropenia / death): 24.0% vs 64.1% (p < 0.00001)
PSA ≤ 0.2 ng/mL: 41.3% vs 48.8%
Same control, less toxicity.
ARASAFE shows bi-weekly 50 mg/m².
Docetaxel + Darolutamide may become the new safer triplet standard in mHSPC ??.”

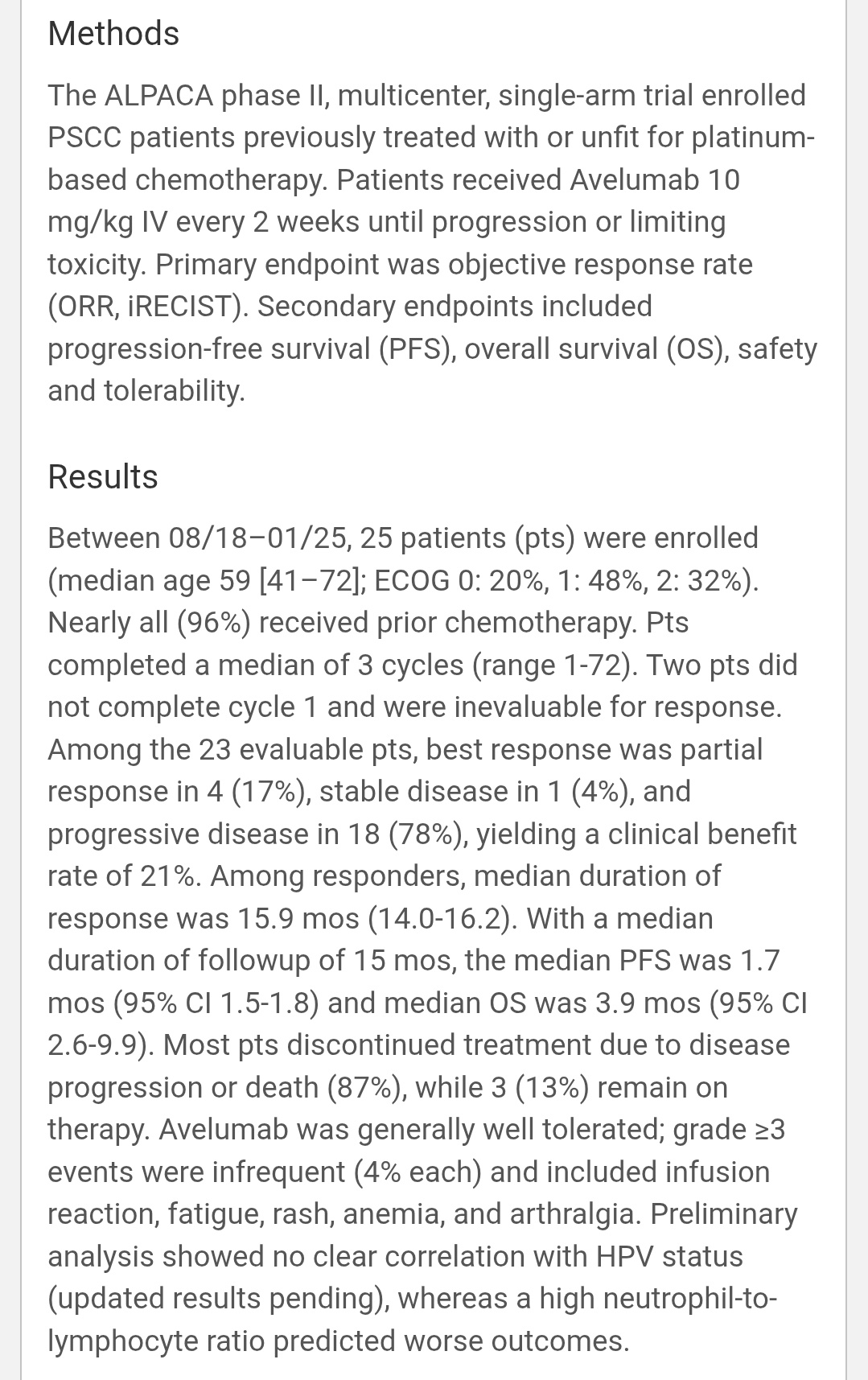
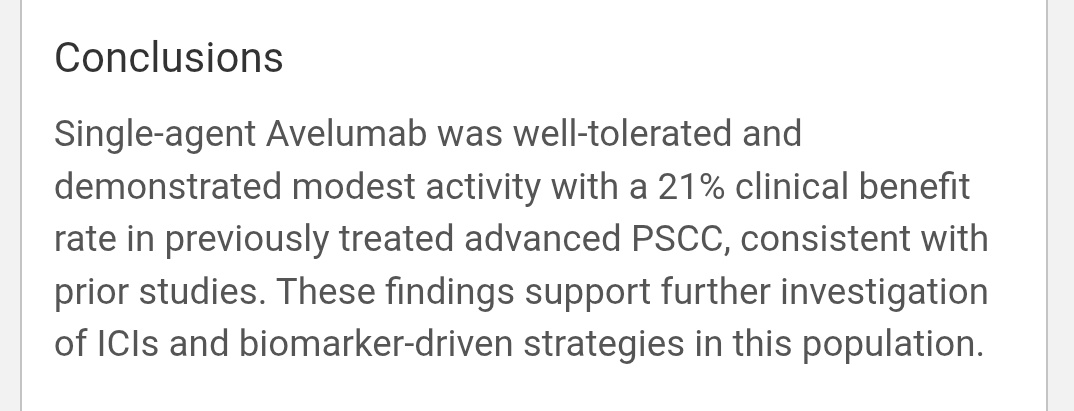
“LBA37 | ALPACA trial (Phase II)
Single-agent Avelumab in advanced/metastatic penile SCC (platinum-pretreated or unfit).
- ORR: 17% (4/23)
- Clinical benefit rate: 21%
- Median DoR: 15.9 mo
- Median PFS: 1.7 mo | OS: 3.9 mo
Well-tolerated; grade ≥3 AEs only ~4%. High neutrophil-to-lymphocyte ratio → worse outcomes. HPV status not clearly predictive. Modest efficacy but durable responses in a rare, hard-to-treat cancer.
Next step → biomarker-driven or combo ICI strategies.”

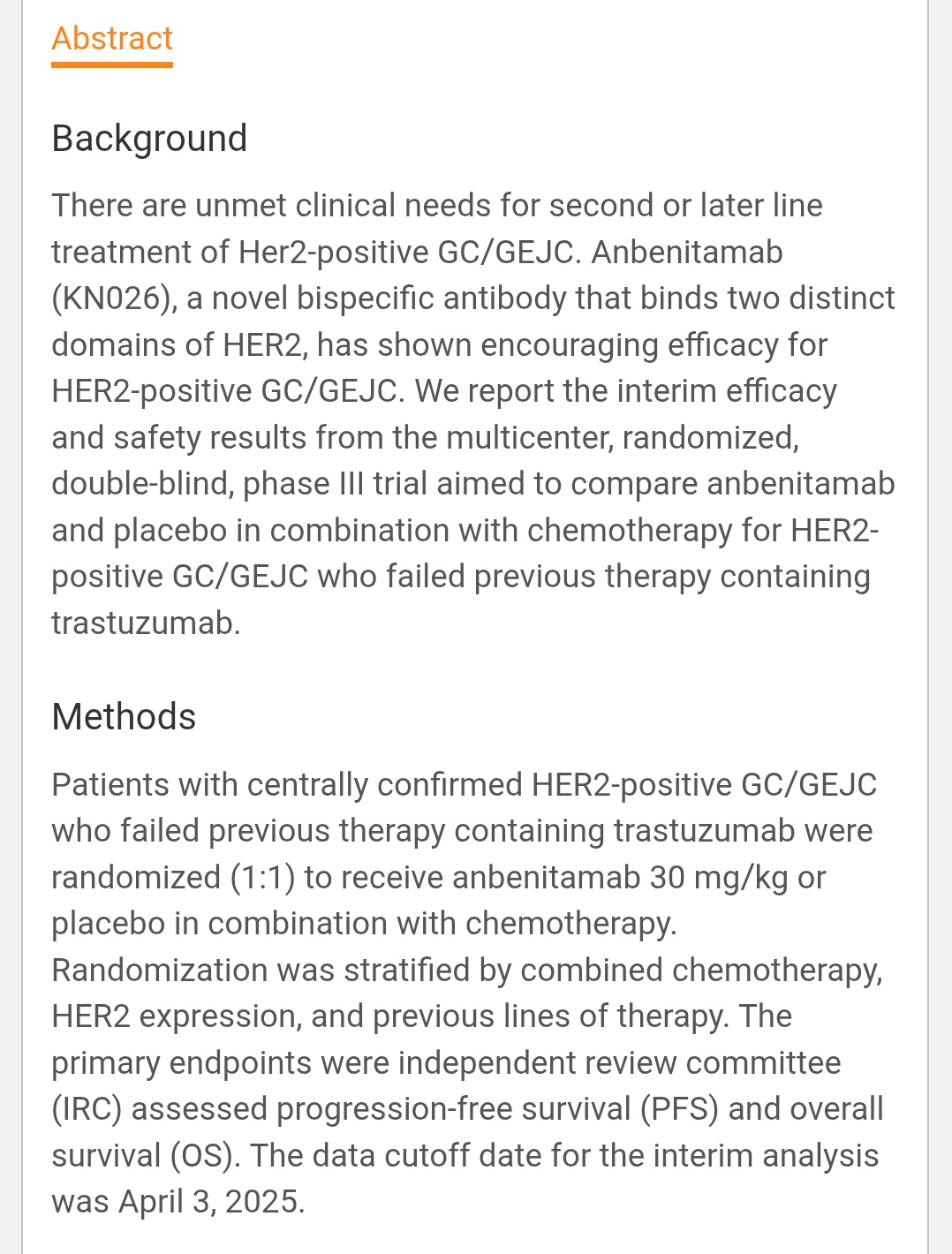
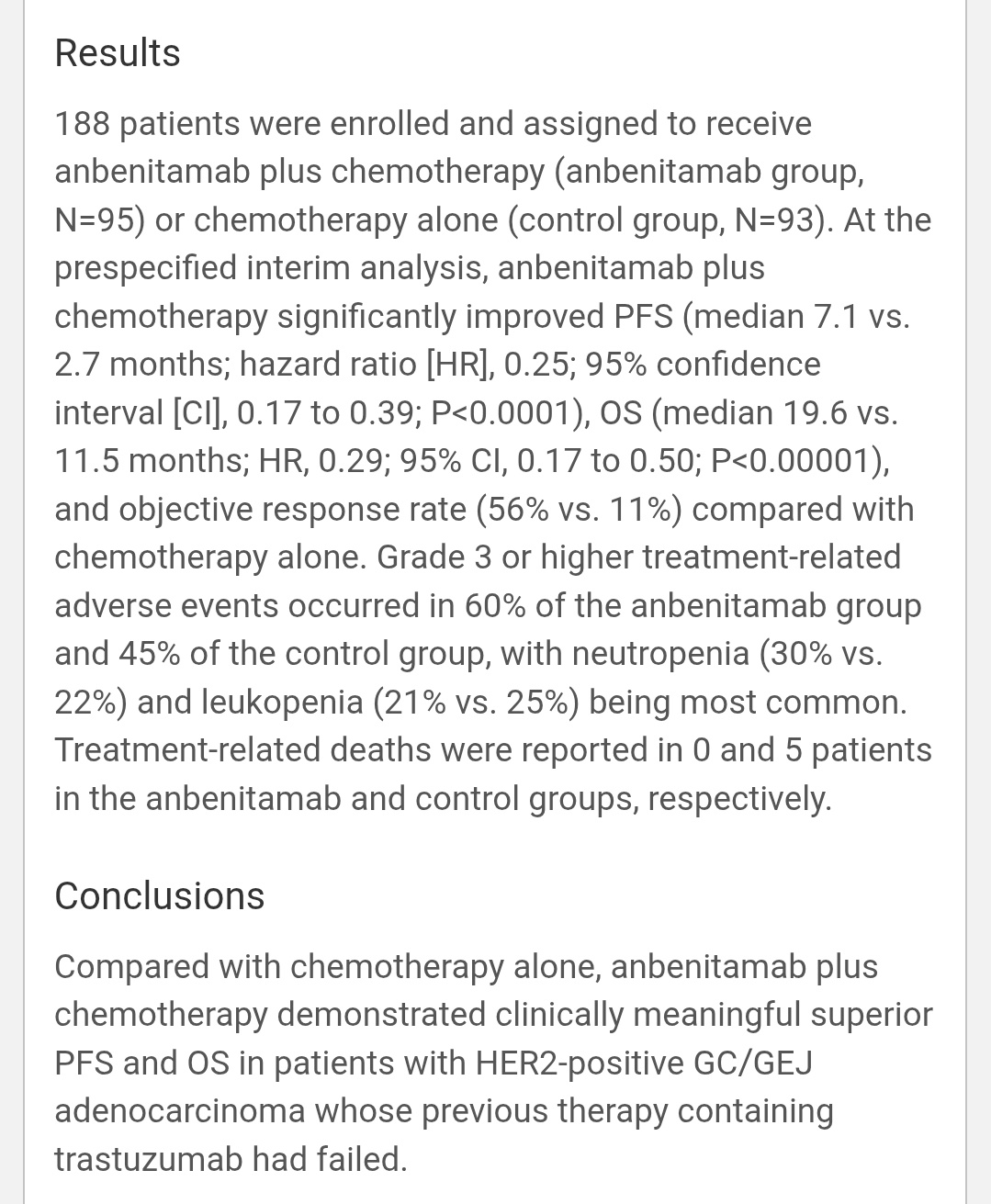
(Anbenitamab) + Chemo in HER2⁺ Gastric/GEJ Cancer After trastuzumab failure, adding Anbenitamab (KN026) — a bispecific HER2 antibody targeting two non-overlapping HER2 epitopes (trastuzumab- & pertuzumab-like) — delivered impressive gains.
PFS: 7.1 mo vs 2.7 mo → HR 0.25
OS: 19.6 mo vs 11.5 mo → HR 0.29
ORR: 56% vs 11% n = 188 (post-trastuzumab, randomized 1:1)
Toxicity: G3+ AEs 60% (vs 45%), mainly neutropenia/leukopenia; no ILD signal
Dual HER2 blockade in one molecule = powerful & practical alternative where T-DXd is limited?”

Lenvatinib + Pembrolizumab + Chemo vs Pembrolizumab + Chemo in 1L mESCC
No OS benefit
Median OS 17.6 vs 15.5 mo | HR 0.92 (p = 0.18)
PFS 7.2 vs 6.9 mo | ORR 62 % vs 55 %
AE ≥ G3 ≈ 69 % each
Study stopped early – no chance of significance.
Pembrolizumab + chemo remains standard. Another VEGF + IO combo fails to lift the curve.”

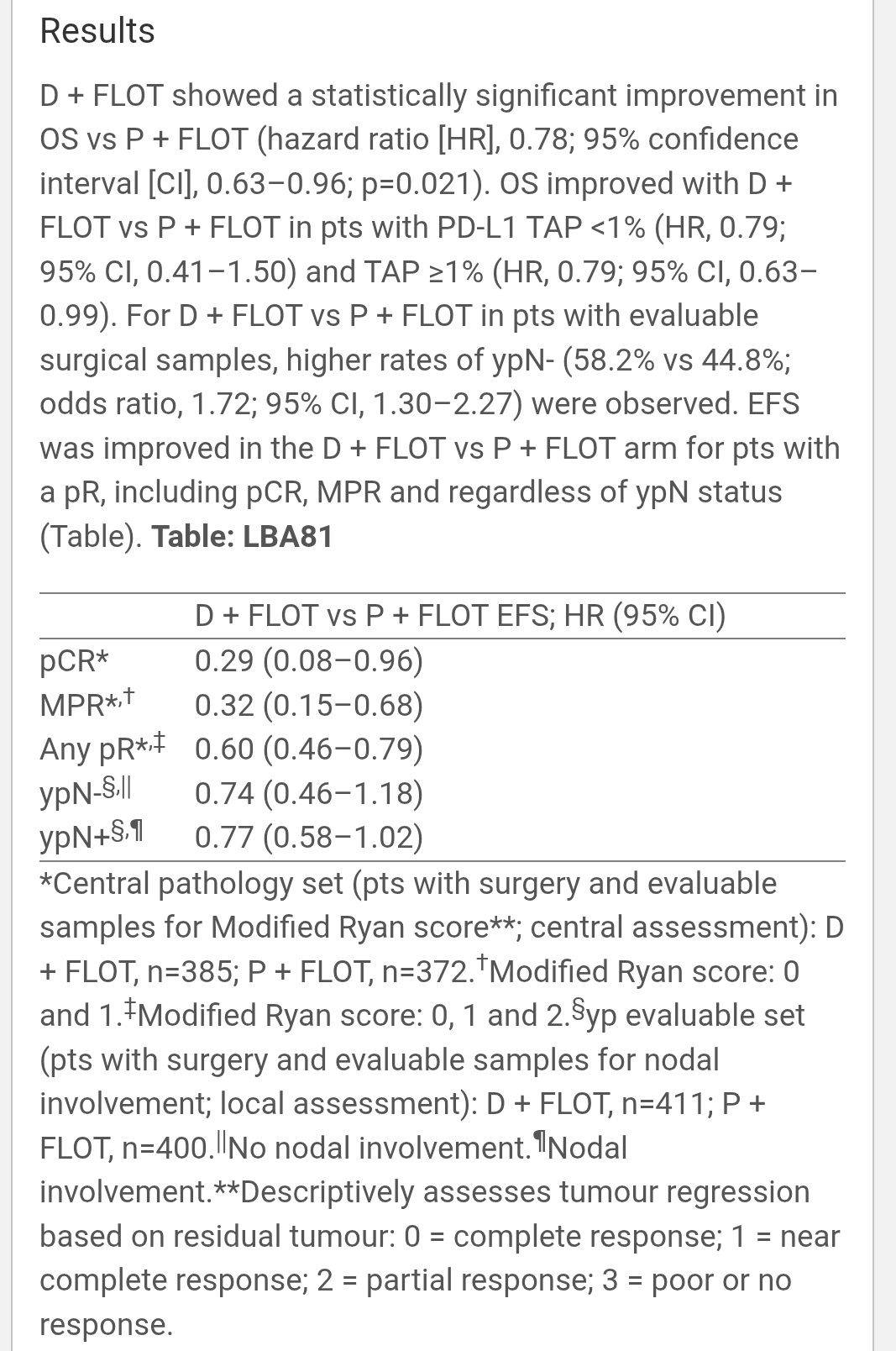
Durvalumab + FLOT vs Placebo + FLOT in resectable gastric / GEJ adenocarcinoma.
Final OS positive — first peri-operative gastric study showing OS gain with IO + FLOT
Key results:
OS HR 0.78 (95% CI 0.63–0.96, p = 0.021)
Benefit consistent across PD-L1, but CIs > 1 in some subgroups
- TAP < 1 % HR 0.79 (0.41–1.50) — NS
- TAP ≥ 1 % HR 0.79 (0.63–0.99) borderline
Pathologic responses:
- pCR 0.29 (0.08–0.96)
- MPR 0.32 (0.15–0.68)
- Any pR 0.60 (0.46–0.79)
- ypN– 0.74 (0.46–1.18) NS
- ypN+ 0.77 (0.58–1.02) NS
ypN– downstaging: 58.2 % vs 44.8 % (OR 1.72)
Takeaway:
- Significant OS & pathological response gains,
- Some subgroups CIs cross 1 → interpret cautiously,
- Peri-operative Durvalumab + FLOT emerges as new SOC.”

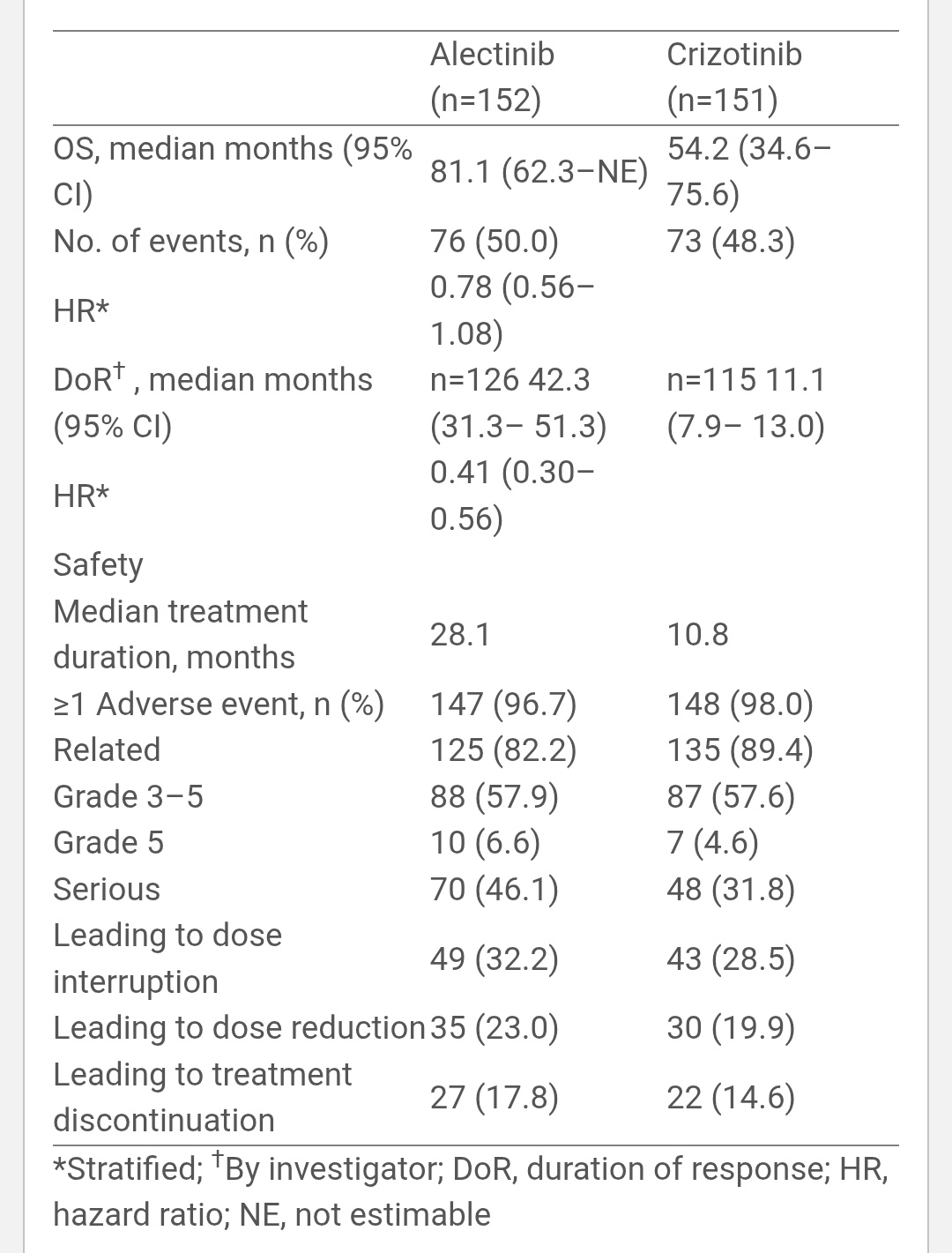
“LBA73 – Final ALEX OS Update.
1L ALK+ NSCLC | Alectinib vs Crizotinib
Follow-up: 53.5 mo (Alec) vs 23.3 mo (Crizo)
Median OS: 81.1 mo vs 54.2 mo → HR 0.78 (0.56–1.08)
Median DoR: 42.3 mo vs 11.1 mo → HR 0.41 (0.30–0.56)
CNS benefit:
• With prior RT 92 vs 39.5 mo
• Without RT 46.9 vs 23.7 mo
• No CNS mets 94 vs 69.8 mo
Safety: Similar Grade 3–5 AEs (58% vs 58%), no new signals.
Takeaway: Final ALEX confirms durable OS ≈ 6.8 years with alectinib, deep & prolonged responses, and sustained CNS protection.
Still the global benchmark for 1L ALK+ NSCLC – setting the bar high for next-gen TKIs.”

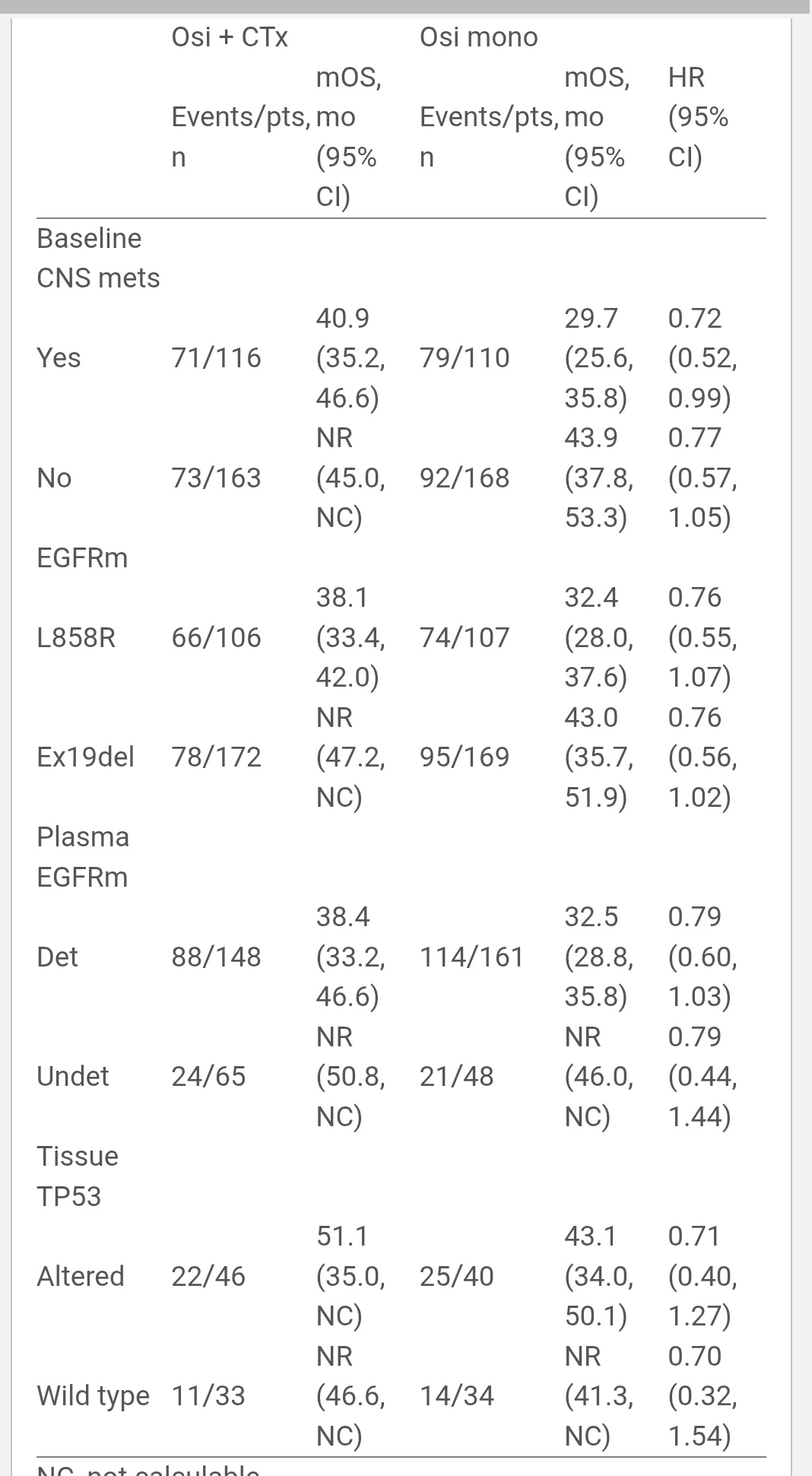
“FLAURA2 (LBA77).
Final OS confirms it — Osimertinib + platinum-pemetrexed > Osimertinib alone in 1L EGFR-mutant NSCLC.
HR 0.77 | p = 0.02 Across poor-risk subgroups:
CNS mets → mOS 40.9 vs 29.7 mo (HR 0.72)
TP53 mut → 51.1 vs 43.1 mo (HR 0.71)
L858R & Ex19del → consistent benefit Survival advantage in every subgroup → combo now clear 1L SOC.”

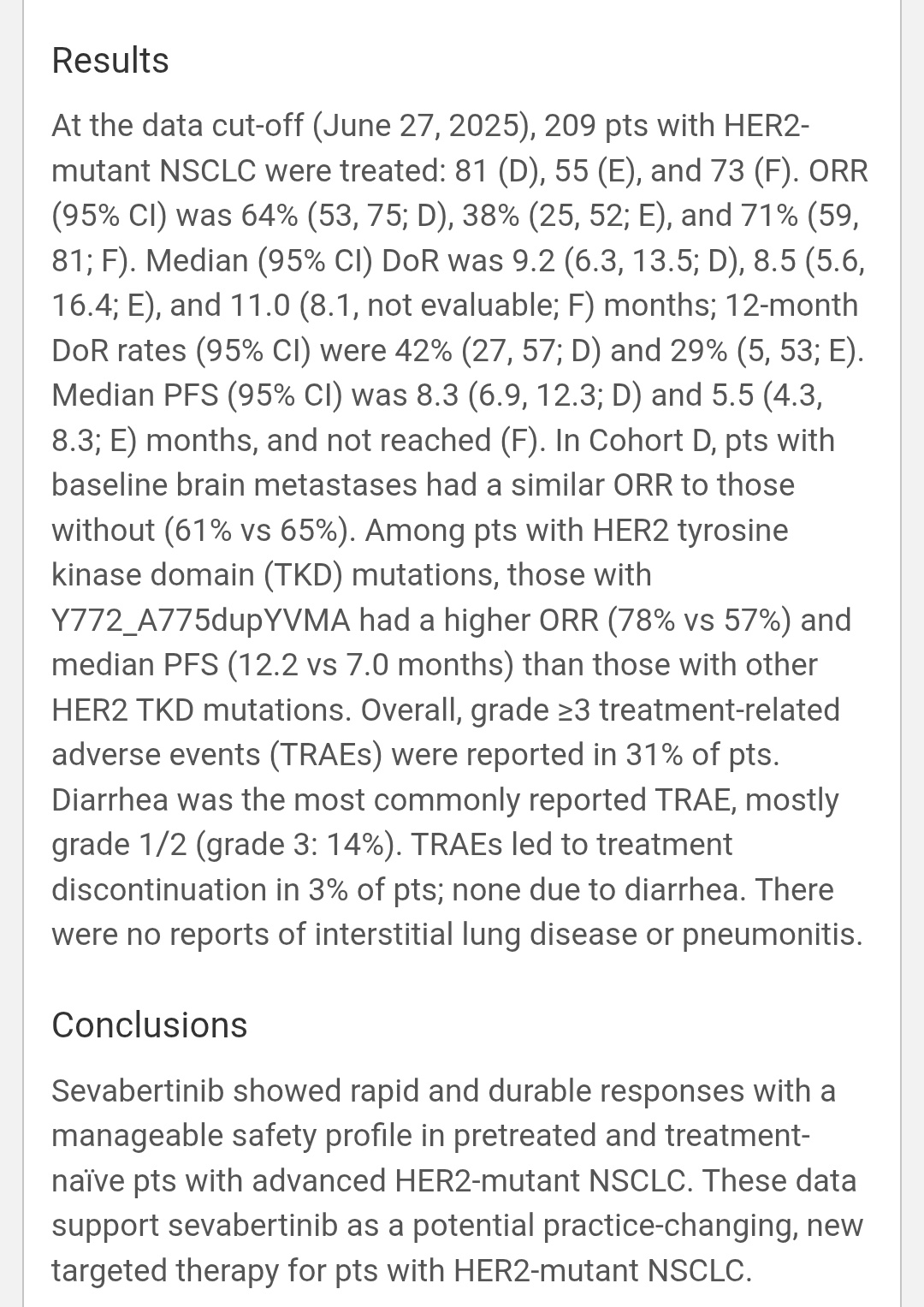
“Sevabertinib in HER2-mutant NSCLC – SOHO-01 ESMO25
Oral, reversible HER2 TKI 209 pts | Phase I/II | NCT05099172
ORR:
• 64% pretreated (D)
• 38% post-ADC (E)
• 71% treatment-naïve (F)
DoR: 9–11 mo
PFS: 8–12 mo (NR in naïve cohort)
Active in brain mets (61% vs 65%).
Best outcomes in HER2 TKD Y772_A775dup (ORR 78%, PFS 12.2 mo)
Well-tolerated, no ILD, grade ≥3 AEs 31% Practice-changing oral HER2 TKI—may redefine care in HER2-mutant NSCLC.”

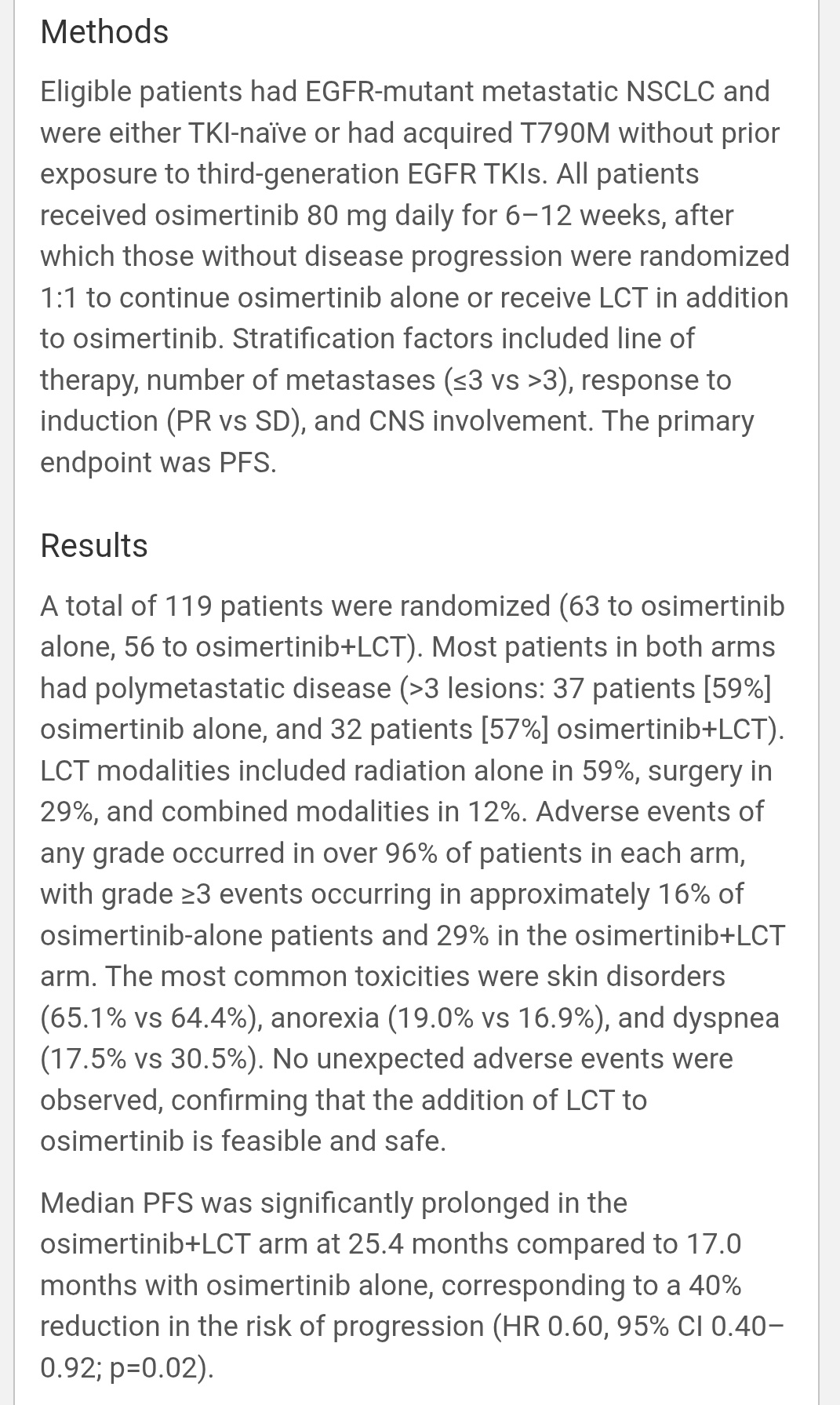
Phase II trial tested osimertinib ± local consolidative therapy (LCT) in EGFR-mutant metastatic NSCLC.
Design: Osimertinib for 6–12 wk non-progressors randomized (1:1) to continue OSI vs OSI + LCT (RT / surgery / both). N = 119 (59 % polymetastatic, 30 % CNS +).
Primary EP: PFS.
Results:
• Median PFS 25.4 mo (OSI + LCT) vs 17.0 mo (OSI alone)
• HR 0.60 (95 % CI 0.40–0.92, p = 0.02)
• Grade ≥ 3 AE 16 % vs 29 % – no unexpected toxicity
Implication: Even in polymetastatic EGFR NSCLC, adding LCT yields 40 % lower risk of progression.
Safe + feasible = new paradigm for long-term disease control.”

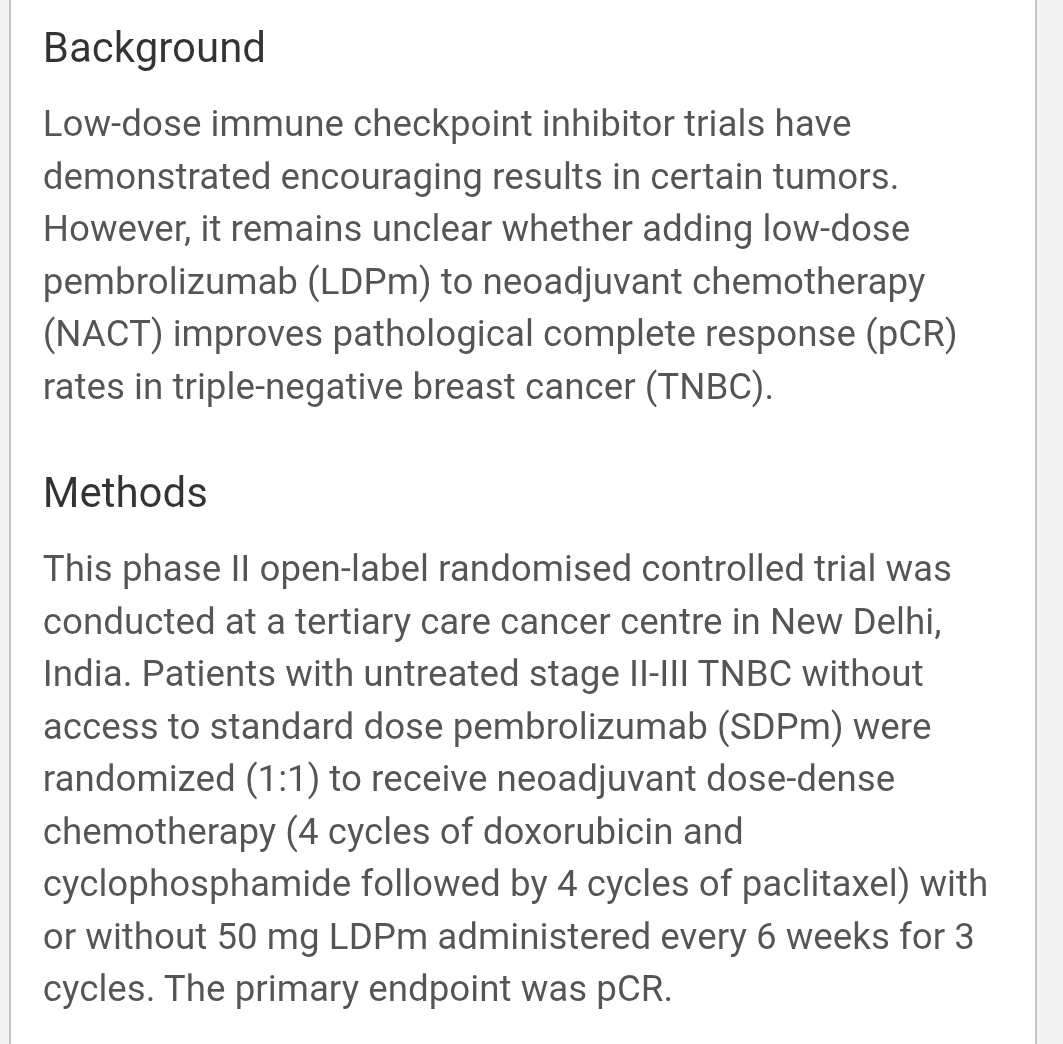
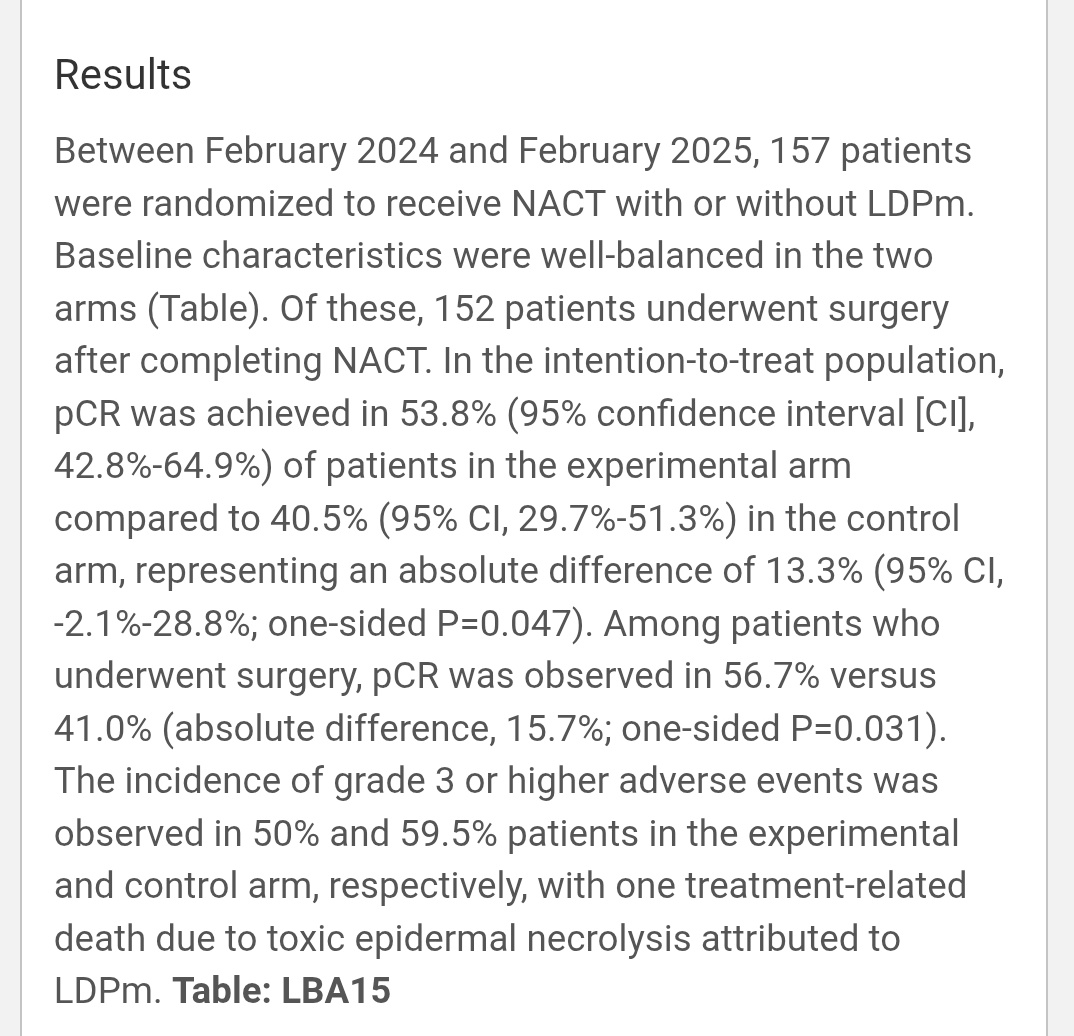
“ESMO 2025 | LBA15 (AIIMS Delhi)
Low-dose Pembrolizumab in TNBC
Phase II RCT: Pembrolizumab 50 mg q6wk × 3 + NACT vs NACT alone
pCR 53.8% vs 40.5% (Δ 13.3%, p = 0.047)
Nearly matches KN-522 results at a fraction of the dose and cost.
Grade ≥ 3 AEs: 50% vs 59.5% Funded by ICMR | Conducted at AIIMS New Delhi
Conclusion: Low-dose pembrolizumab shows comparable efficacy to standard dosing with manageable toxicity. In LMICs, this could be a viable, affordable immunotherapy pathway.”

Read More Live Updates from ESMO25 here.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}