


Fresh from the podium at ESTRO 2025, Dr. Adrian Murray Brunt shared the eagerly awaited 10-year results from the FAST-Forward trial—a practice-changing study that has already reshaped the global standard for adjuvant breast radiotherapy. The trial tested two ultra-hypofractionated 1-week schedules (26 Gy and 27 Gy in five fractions) against the conventional 3-week regimen of 40 Gy in 15 fractions. The new long-term data further solidify 26 Gy in five daily fractions over one week as a safe, effective, and convenient standard for patients with early-stage breast cancer.
Background of the FAST-Forward trial
Adjuvant radiotherapy significantly reduces local recurrence and improves survival in early-stage breast cancer. For decades, the standard UK regimen was 50 Gy in 25 fractions over 5 weeks. This changed after the UK START trials, which demonstrated that 40 Gy in 15 fractions over 3 weeks was equally effective with fewer side effects.
That 3-week schedule became the UK standard in 2009 and is now widely adopted internationally. Building on this progress, the FAST-Forward trial (ISRCTN19906132) tested whether radiotherapy could be safely condensed into 5 fractions over 1 week, offering even greater convenience for patients and health systems.

In the original 5-year results, published in The Lancet in 2020 (Brunt et al.), the trial randomized 4096 patients with early breast cancer (pT1–3, pN0–1, M0) to one of three regimens:
- 40 Gy in 15 fractions over 3 weeks (control).
- 27 Gy in 5 fractions over 1 week.
- 6 Gy in 5 fractions over 1 week.
Key 5-year findings
Ipsilateral breast tumor relapse (primary endpoint)
- 2.1% in the 40 Gy group.
- 1.7% in the 27 Gy group.
- 1.4% in the 26 Gy group.
- Both test arms met the predefined non-inferiority margin (≤1.6% excess relapse allowed vs. control).
- Normal tissue effects (clinician-reported, 5-year prevalence).
- Higher with 27 Gy (15.4%) vs. 40 Gy (9.9%).
- Comparable for 26 Gy (11.9%) vs. 40 Gy.
Again, more adverse effects were seen with 27 Gy; outcomes with 26 Gy were similar to 40 Gy. These results led to a strong consensus that 26 Gy in 5 fractions delivers equivalent cancer control and comparable late toxicity to 40 Gy in 15 fractions. UK national guidelines (NICE) and international recommendations (e.g., ASTRO) began endorsing the 1-week regimen soon after.
What’s new: 10-year outcomes
Dr. Brunt’s ESTRO 2025 presentation delivered on the final co-primary aim: establishing long-term safety and efficacy over a full decade of follow-up.
Results
FAST-Forward trial confirming that a one-week ultra-hypofractionated radiotherapy schedule (26 Gy in 5 fractions) offers equivalent or better outcomes compared to the standard 3-week regimen (40 Gy in 15 fractions). The results demonstrate excellent long-term local control, minimal late toxicity, and comparable survival outcomes, supporting a major shift in global radiotherapy practice for early breast cancer.
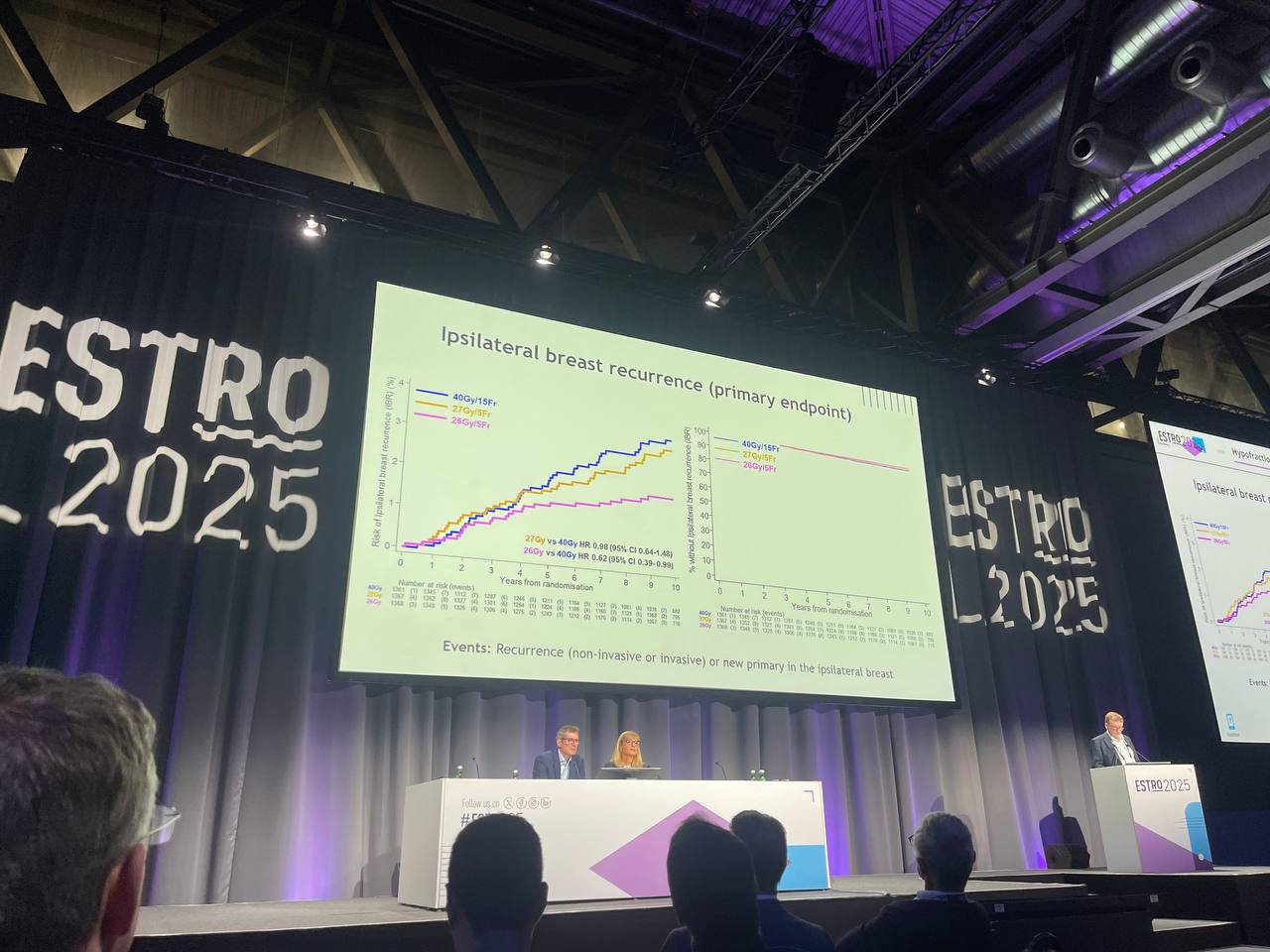
Local Control. 10-year ipsilateral breast tumor recurrence (IBTR):
- 40 Gy (control): 3.6%
- 27 Gy: 3.0%
- 26 Gy: 2.0%

Hazard ratio (26 Gy vs. 40 Gy): 0.62 which indicates non-inferiority and a trend toward superiority of 26 Gy
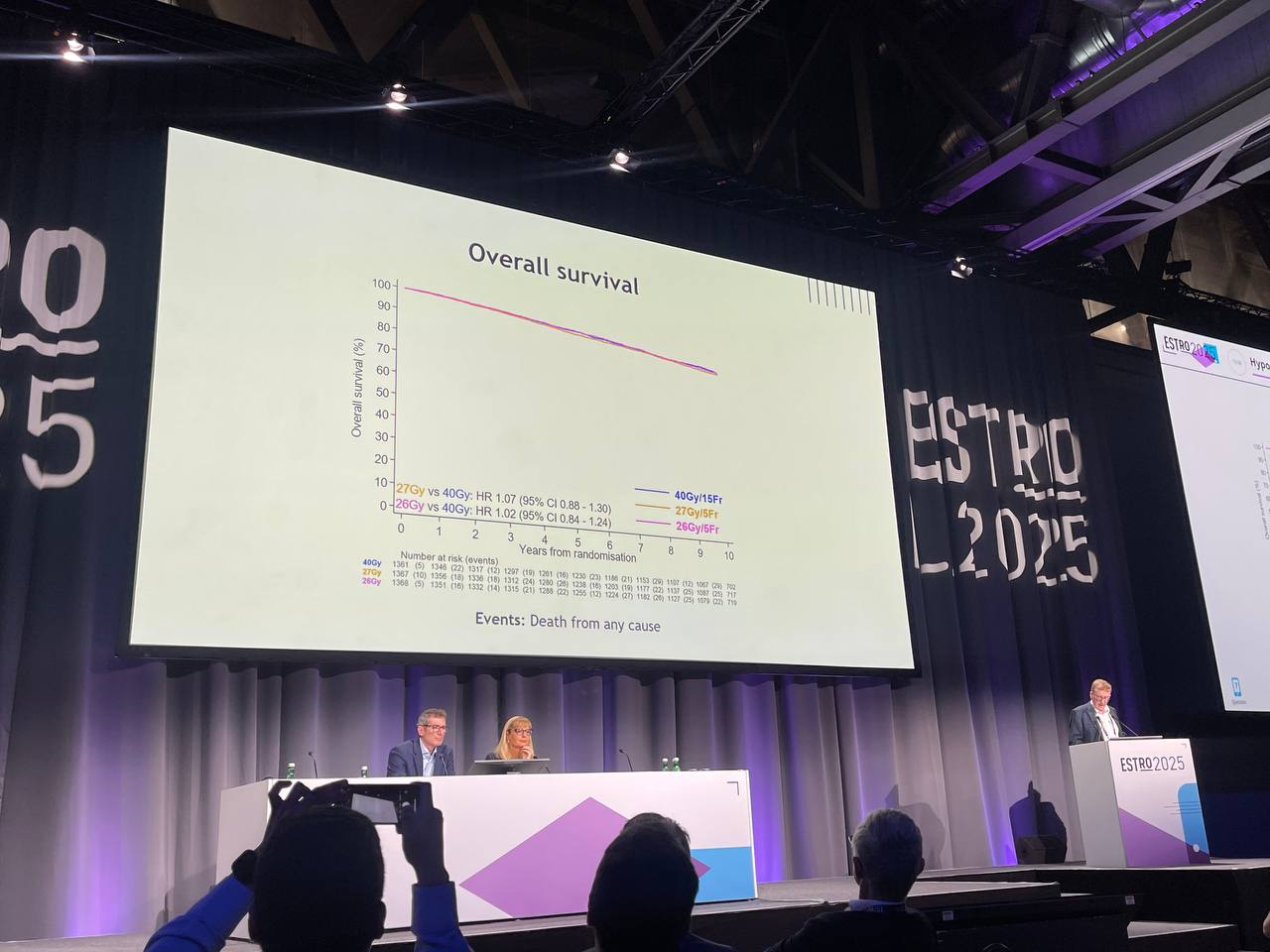
Overall survival and breast cancer-specific survival was similar across all three treatment arms. Distant recurrence, second primary tumors, and contralateral breast cancers showed no increased incidence in either hypofractionated group compared to the standard regimen.
Late Normal Tissue Effects. Clinician-reported (10-year assessment):
- 26 Gy: Comparable to 40 Gy.
- 27 Gy: Higher rates of firmness, shrinkage, and induration.
- Patient-reported outcomes (breast symptoms, appearance, swelling).
- 26 Gy: Very similar to 40 Gy.
- 27 Gy: Slightly worse outcomes.
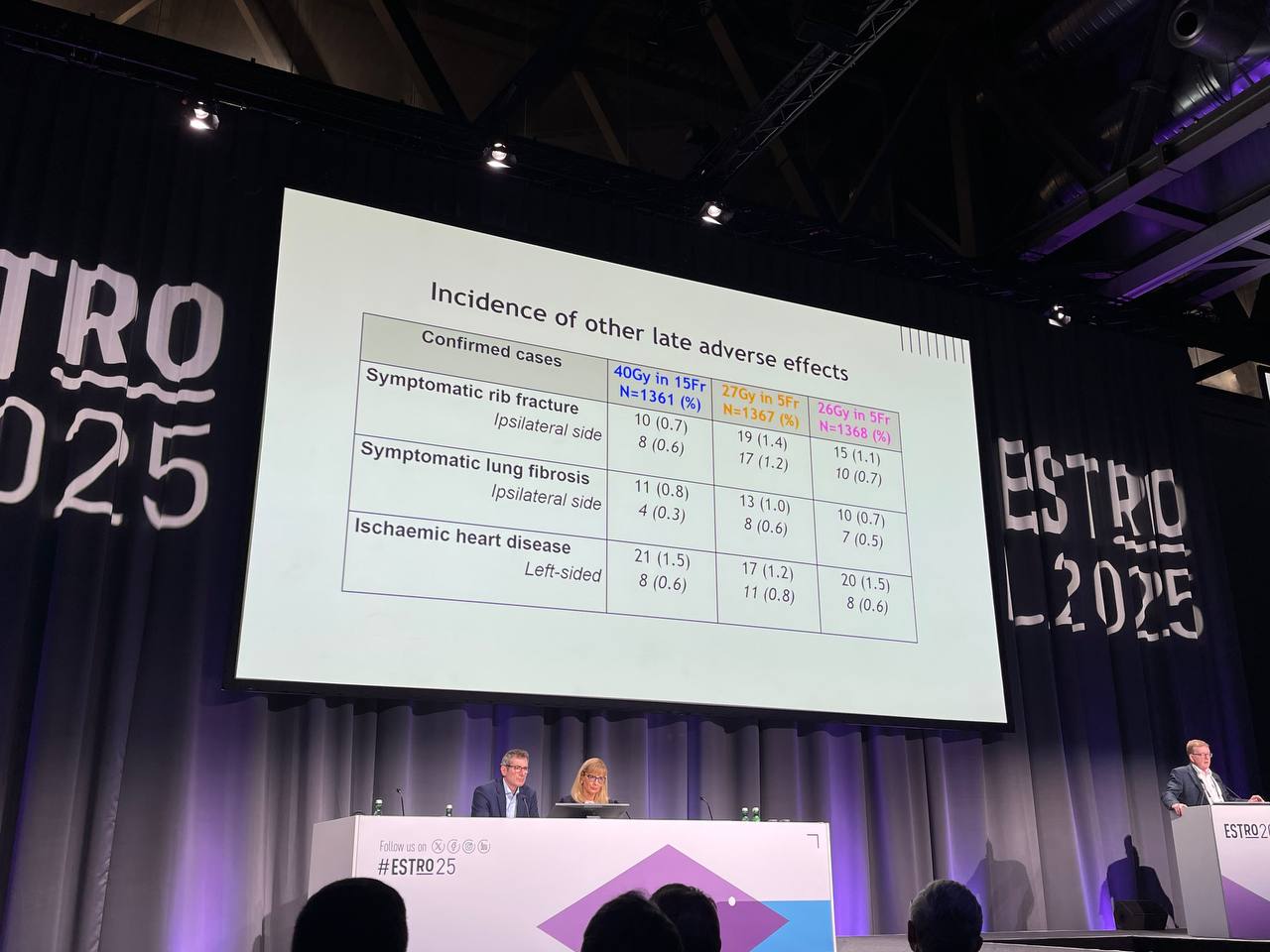
No significant differences in other late adverse effects:
- Rib fractures.
- Symptomatic lung fibrosis.
- Cardiac ischemia.
Key takeaways
FAST-Forward confirms that less might be more: one week of WBI achieves outstanding 10-year outcomes.
- Low incidence of IBR across all schedules.
- Patient and clinician-reported late effects similar for 26Gy/5Fr and 40Gy/15Fr.
- Results confirm 26Gy/5Fr as appropriate SOC.
- Breast.
- Chest wall.
- Partial breast.
- Ongoing analyses will further explore normal tissue effects reported over time.

Read ESTRO 2025 Live Coverage by OncoDaily.
{kind=link}
{kind=link}
{kind=link}