


Manni Mohyuddin shared on X/Twitter:
“Our paper on performance of myeloma staging systems just out:
Thanks to Sam Rubinstein, Vincent Rajkumar and Rafael Fonseca for their mentorship/support on this piece.
Here is a thread on this paper and staging/risk stratification in myeloma.
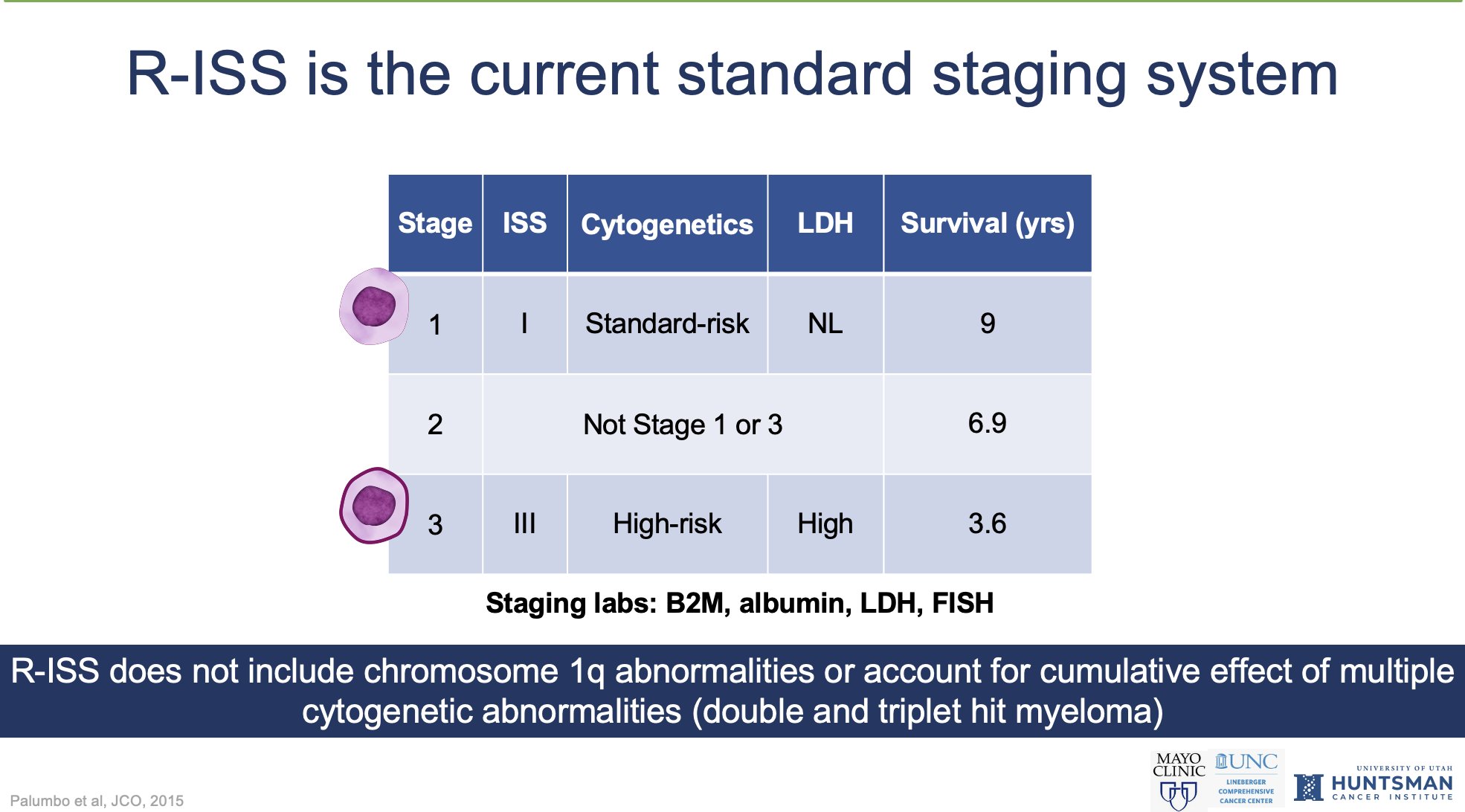
The R-ISS is most commonly used staging system.
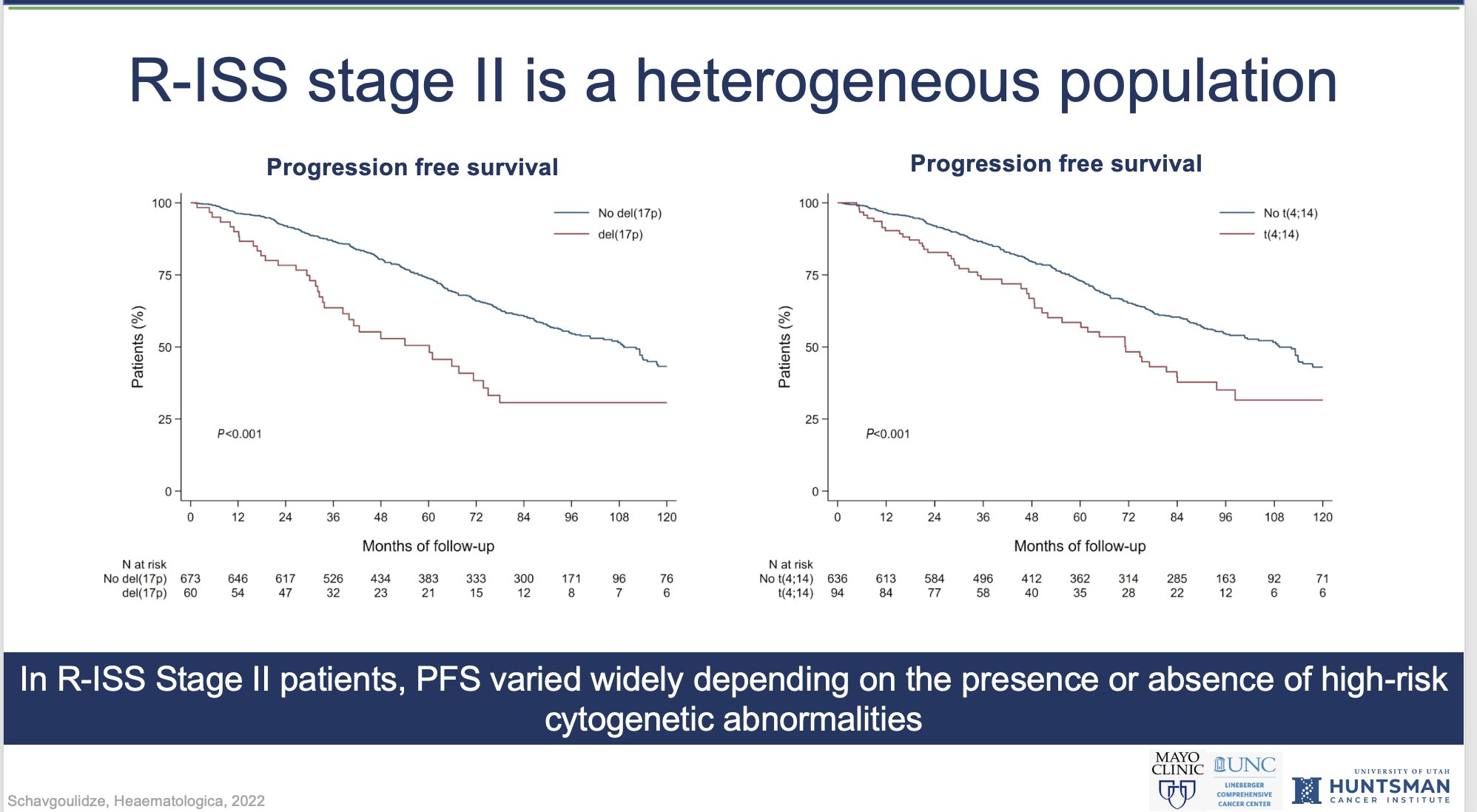
One of the problems with R-ISS, is that the majority of patients end up being stage 2, and Stage 2 can have incredible heterogeneity, as people with 0, 1 or 2 high-risk cytogenetics all can be Stage 2!
Visit the article website.
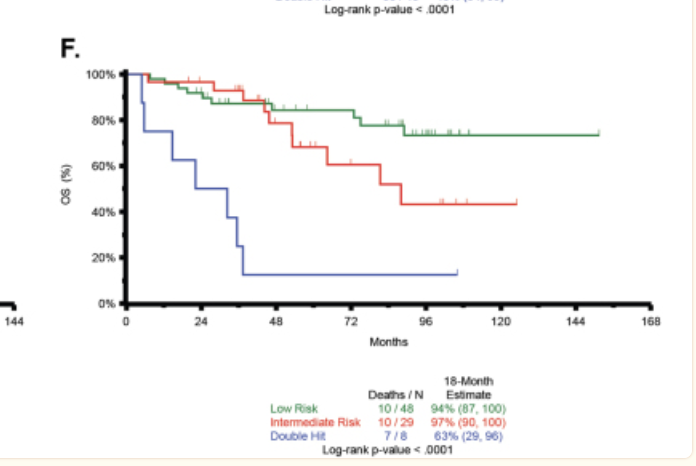
A seminal paper in the understanding of risk in myeloma was the observation that having multiple high-risk cytogenetic abnormalities contributes to an additive risk of progression/death.
This was not accounted for in R-ISS, a key limitation.
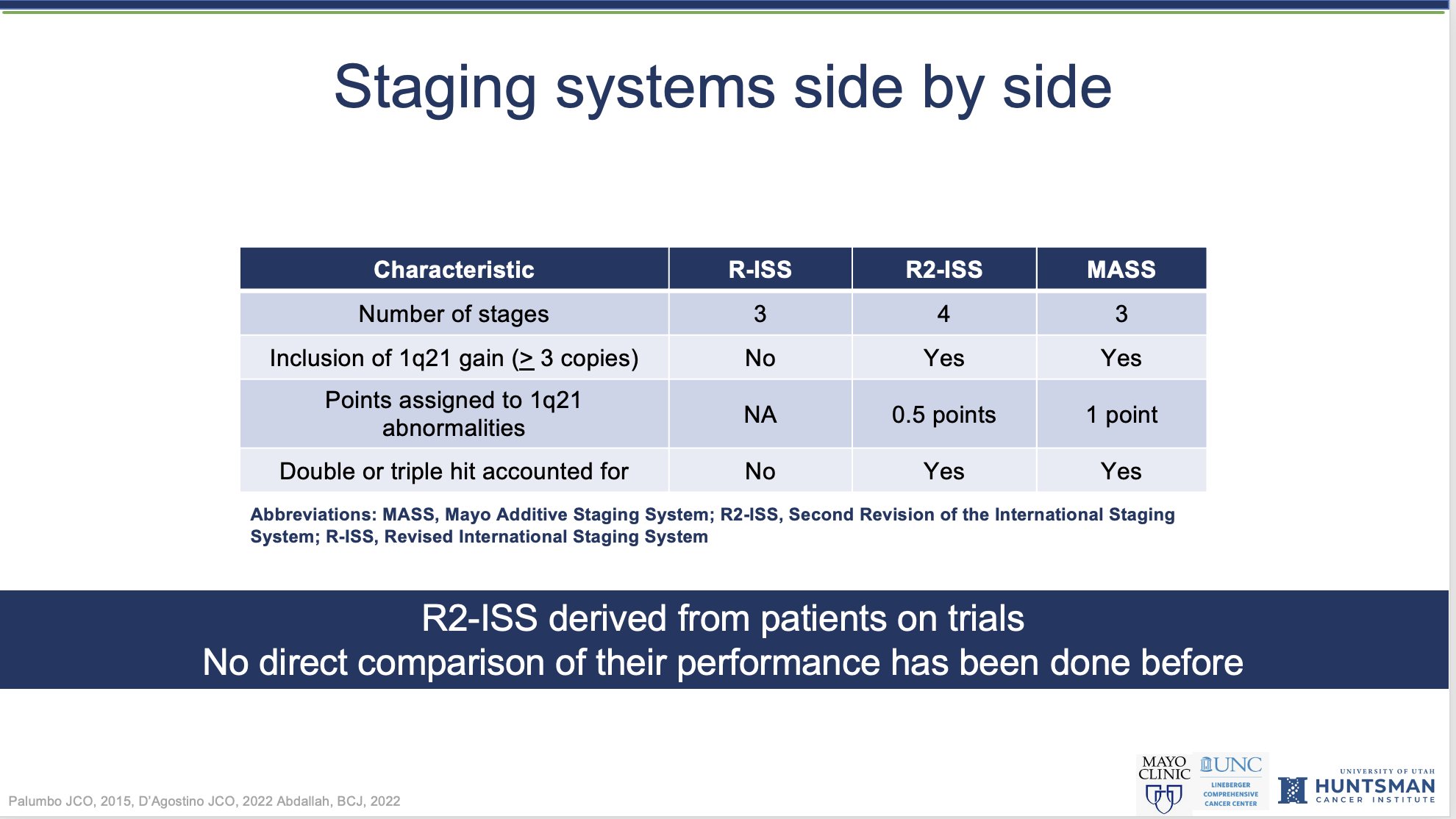
Two new staging systems, MASS and R-2 ISS have aimed to address these deficiencies.
They are both similar in that regard- with some differences in weightage.
They have never been compared head to head in a large real-world cohort.
Before I describe our results, something about the c-statistic here.
The c-statistic tells us about the performance/predictive ability of a staging system.
A c-statistic of 0.5 is no better than a coin-flip.
More than 0.8 indicates very good performance.
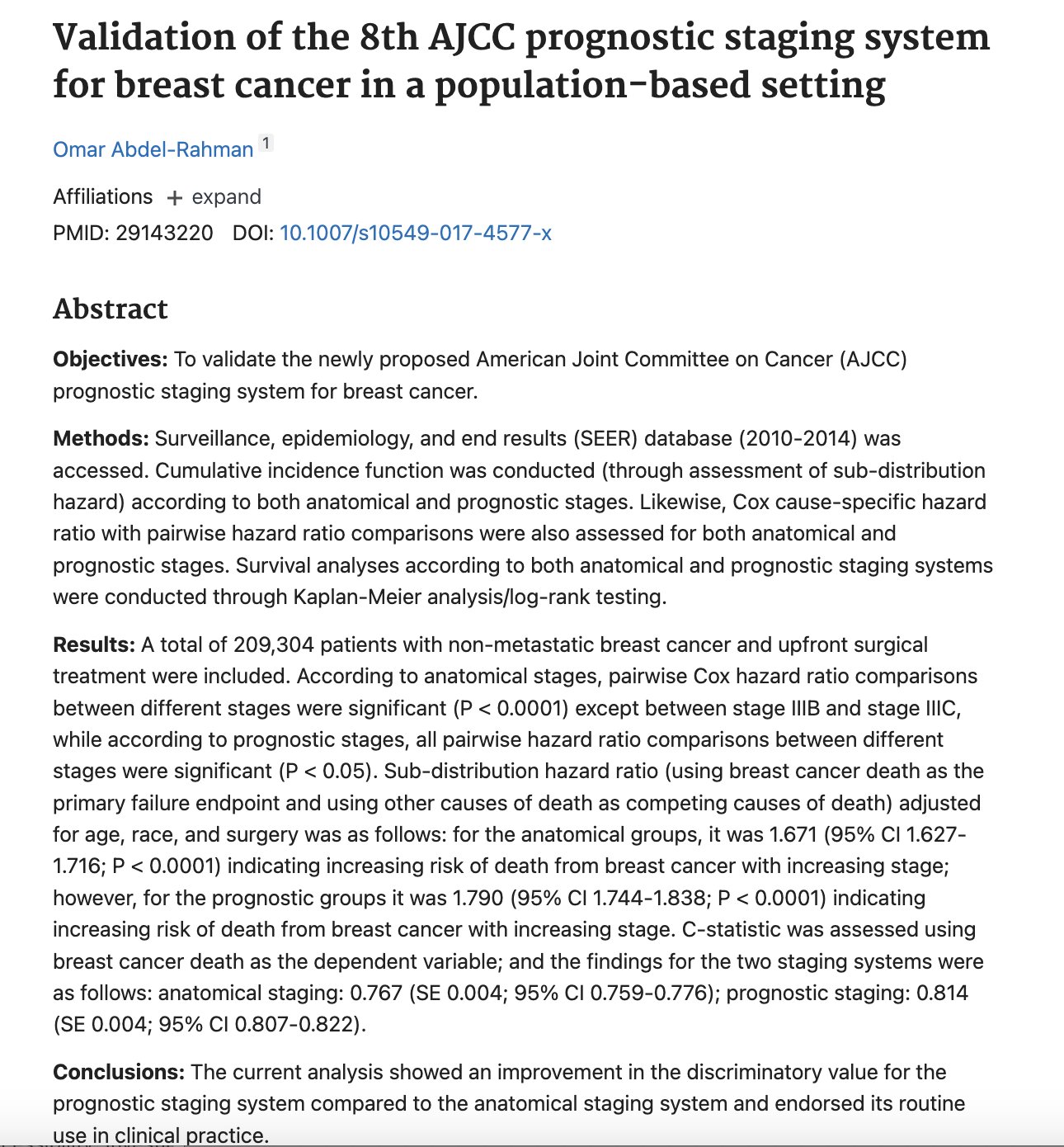
For many solid tumors, a different stage indicates a dramatically different treatment approach (metastasis versus not, local treatments versus systemic treatments) and the c-statistic of staging systems reflects this.
Prognostic staging for breast cancer has c stat of 0.81.

In myeloma, whether one is Stage 1 or Stage 3 does not have a dramatically different approach to treatment (yet), or intent of treatment. It affects prognosis, but perhaps less so than solid tumors.
C-indices of recent staging systems reflects that.
R2-ISS= 0.71
MASS=0.57
As Vincent Rajkumar pointed out, myeloma ‘staging’ systems are a misnomer.
Staging usually reflects tumor burden/spread.
Myeloma staging is a risk stratification that is grouping pts using heterogenous variables, such as biologic aggressiveness, host characteristics, tumor burden.
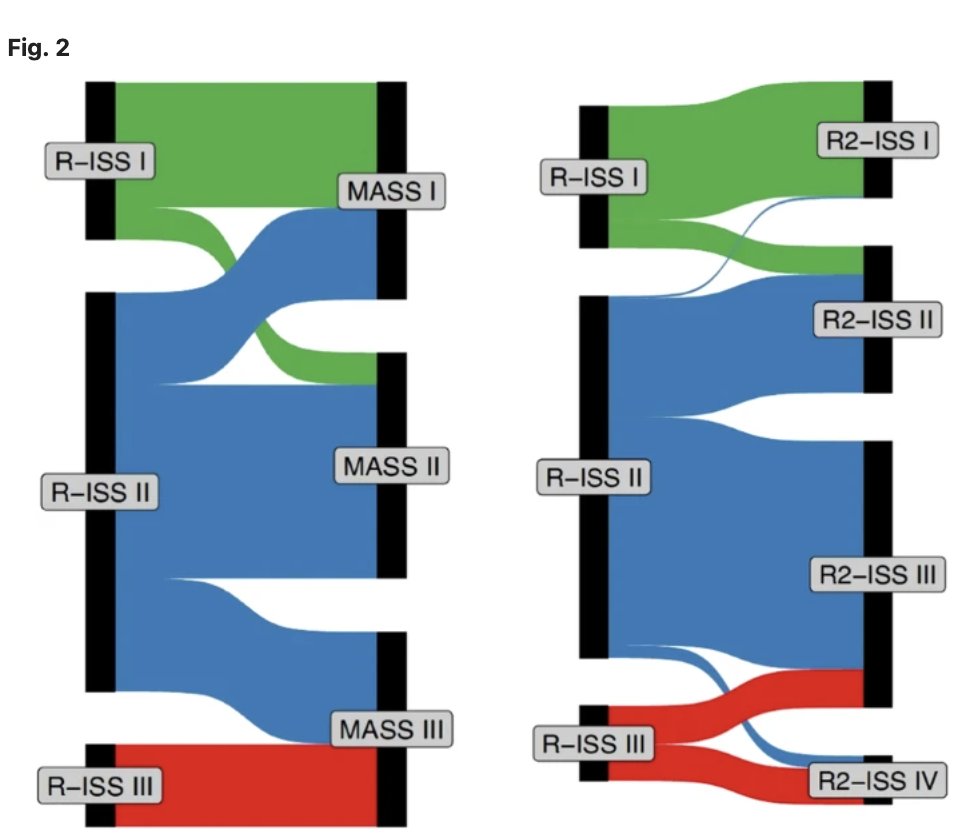
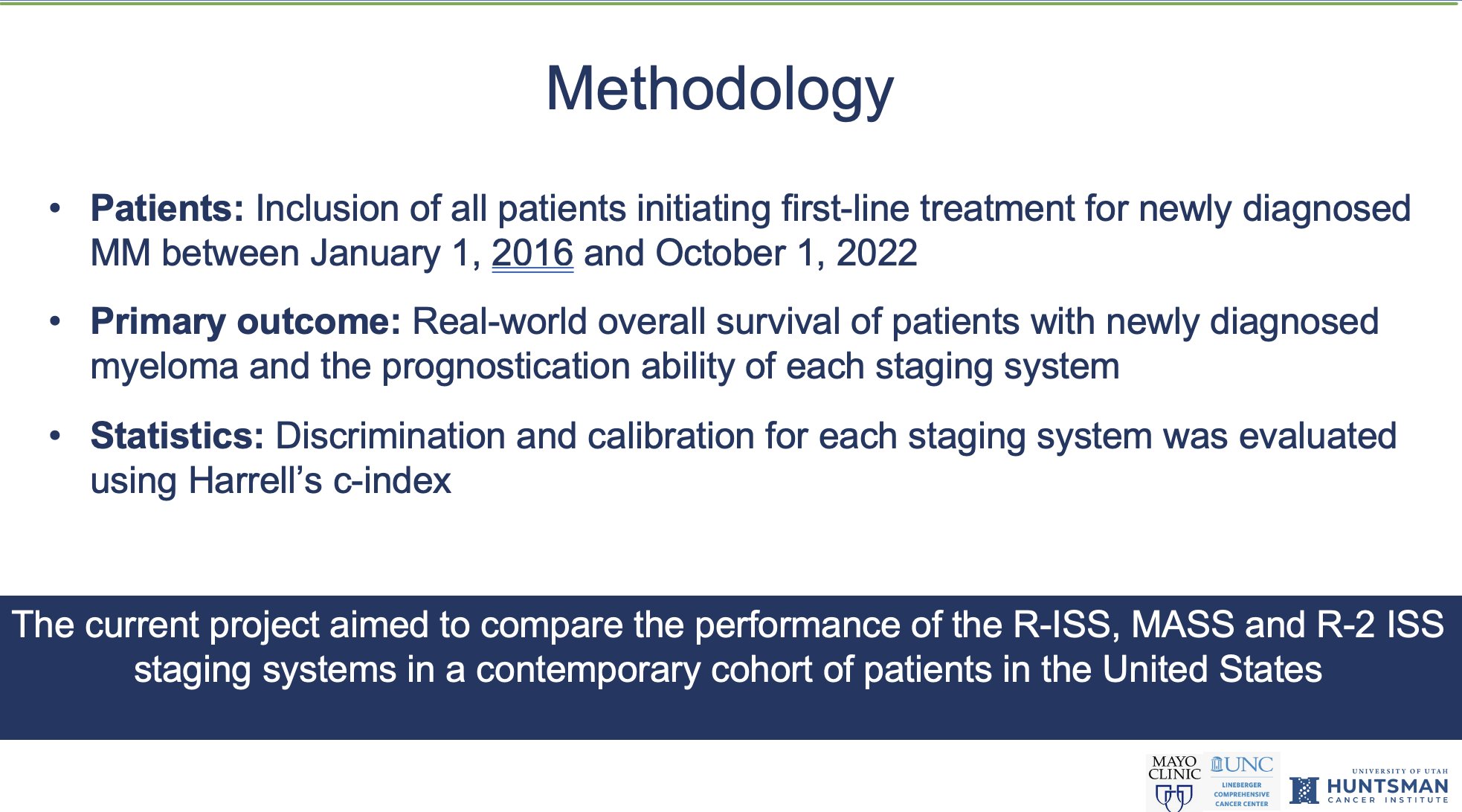
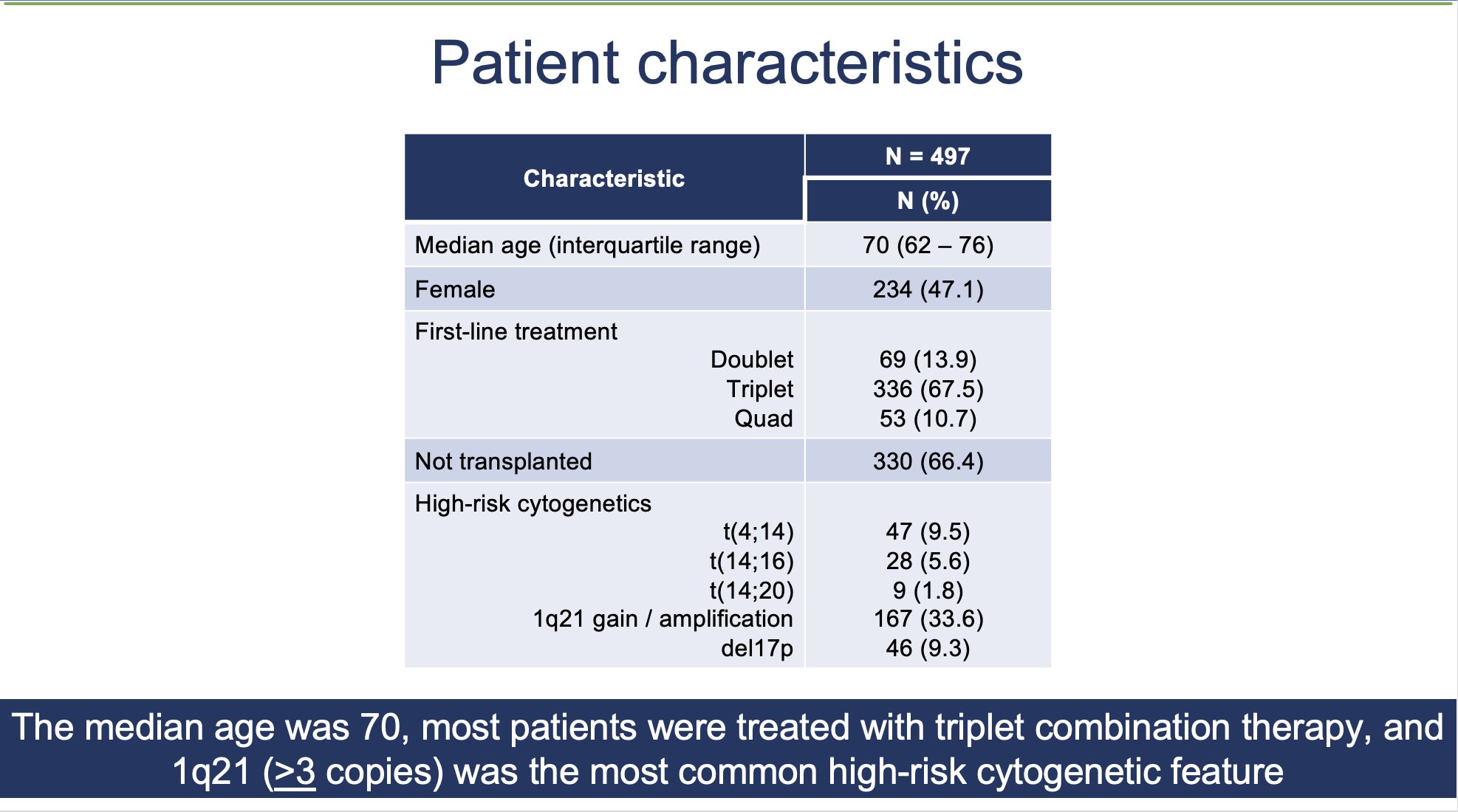
In our paper, we evaluated the performance of R-ISS, MASS and R-2ISS in using the nationwide Flatiron database!
We found out that these newer staging systems, improve upon R-ISS, by redistributing patients from Stage 2 R-ISS into more discrete categories.
You end up with less than a majority of patients in a ‘broad’ stage 2 category. This is their key advantage!
Unfortunately though- the c-statistic for all these staging models (R-ISS, MASS, R2-ISS) remains around 0.6, highlighting room for improvement.
A key limitation of our study is short follow-up (only 23 months), and it is important to analyze with longer-follow-up.
Whats next?
A comprehensive genomic staging was recently published.
This is very thorough, but comes at a cost (I do not/cannot routinely calculate this for all patients I see).
Ideally a staging system should be quick/easy to use and perform well!
Our treatments evolve rapidly, and all risk stratification models are derived from cohorts of patients in the past, who received treatment very different than what we give today or will give years from now.
These models too will continue to evolve, but challenges remain!
Take-home message to clinicians:
-Recognize that staging for myeloma is imperfect, and that R-ISS Stage 2 can have a lot of heterogeneity
-Think of cytogenetic abnormalities, and their additive risk (i.e gain1q+4;14 worse than just one alone)
Thanks for reading!
END.”
Source: Manni Mohyuddin/X

Dr. Manni Mohyuddin is an Assistant Professor at the Huntsman Cancer Institute, University of Utah, specializing in oncology. He is mainly interested in myeloma, supportive care, end-of-life management, and implementing cost-effective, evidence-based treatment strategies.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}