


Menin-dependent transcriptional programs are fundamental to the pathogenesis of NPM1-mutated and KMT2A-rearranged AML, molecular subtypes accounting for approximately 35-40% of AML cases. By regulating genes such as HOXA9 and MEIS1, the menin complex sustains leukemic self-renewal and blocks normal differentiation, providing a strong rationale for therapeutic menin inhibition.
Ziftomenib is a potent, selective oral menin inhibitor approved in the United States for relapsed or refractory NPM1-mutated AML. KOMET-007 is an ongoing, multicenter, open-label phase 1a/b study evaluating ziftomenib-based combinations in NPM1-mutated and KMT2A-rearranged AML.
Presented by Amer M. Zeidan at EHA 2026, this analysis reports updated outcomes from the newly diagnosed cohort receiving ziftomenib in combination with standard 7+3 induction chemotherapy.
Treatment Strategy and Endpoints
Following dose escalation, 600 mg once daily was selected as the recommended phase 2 dose and evaluated in the expansion cohort.
Ziftomenib was initiated on day 8 of induction and continued throughout consolidation and maintenance. Patients could proceed to HSCT when clinically indicated and subsequently resume maintenance therapy.
Primary endpoints included safety and complete remission. Secondary endpoints included CRc, ORR, MRD negativity, DOR, and OS.

Patient Population
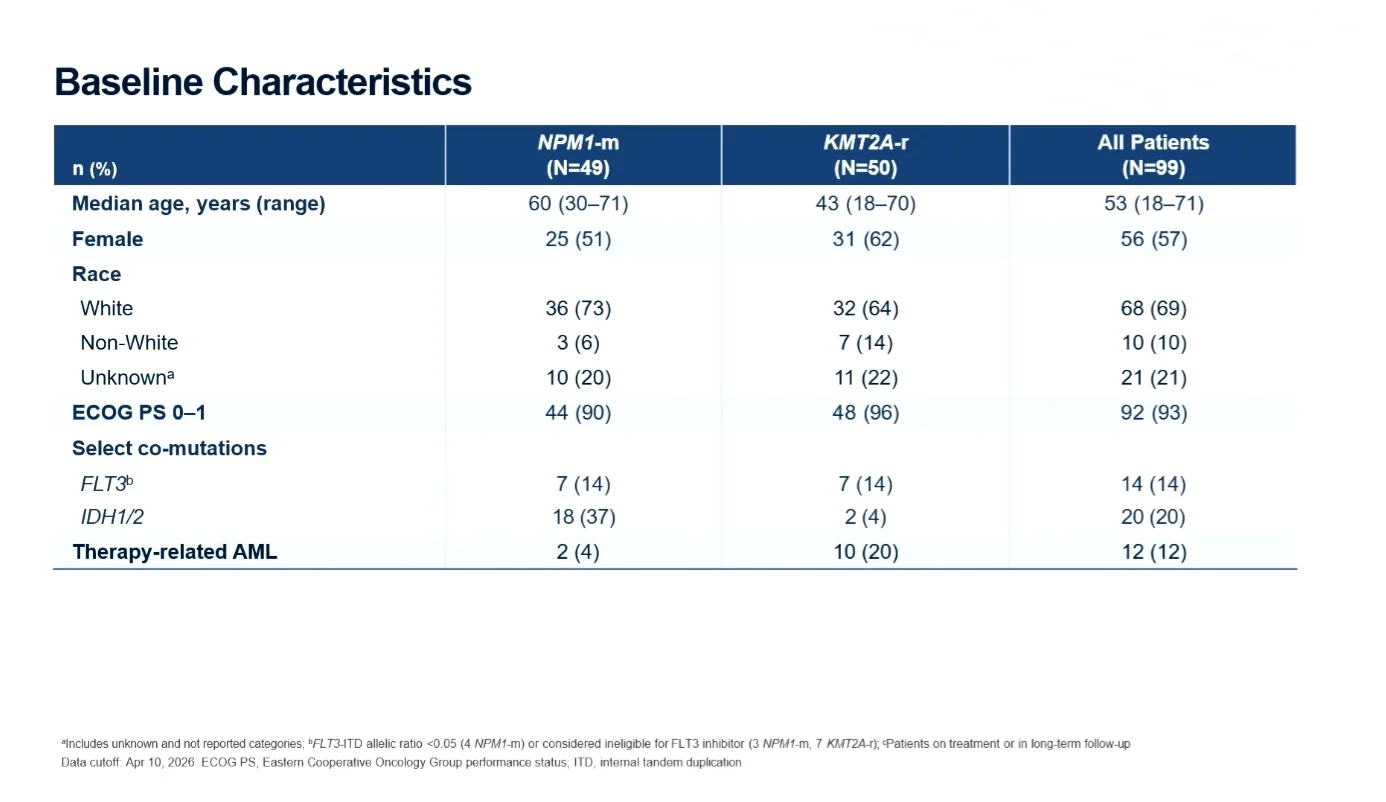
A total of 99 patients were treated with ziftomenib 600 mg plus 7+3, including 49 patients with NPM1-mutated AML and 50 with KMT2A-rearranged AML. The median age was 53 years, and most patients had an ECOG performance status of 0-1.
The NPM1-mutated cohort was generally older and more frequently harbored concurrent IDH1/2 mutations, while therapy-related AML was more common among patients with KMT2A-rearrangement. Follow-up exceeded one year in the NPM1-mutated cohort and approached one year in the KMT2A-rearranged cohort.
Safety and Tolerability
The most common adverse events were predominantly hematologic, alongside gastrointestinal toxicities. The pattern of adverse events was generally similar across both molecular subgroups. Grade ≥3 toxicities were primarily hematologic. Importantly, no new safety signals emerged during prolonged treatment exposure.
Adverse events of special interest were uncommon. Differentiation syndrome occurred in 4% of patients (KMT2A-rearranged cohort), all grade 3 and all successfully managed with protocol-directed interventions. QTc prolongation was infrequent, limited to grade 3 events, and resolved in all affected patients.
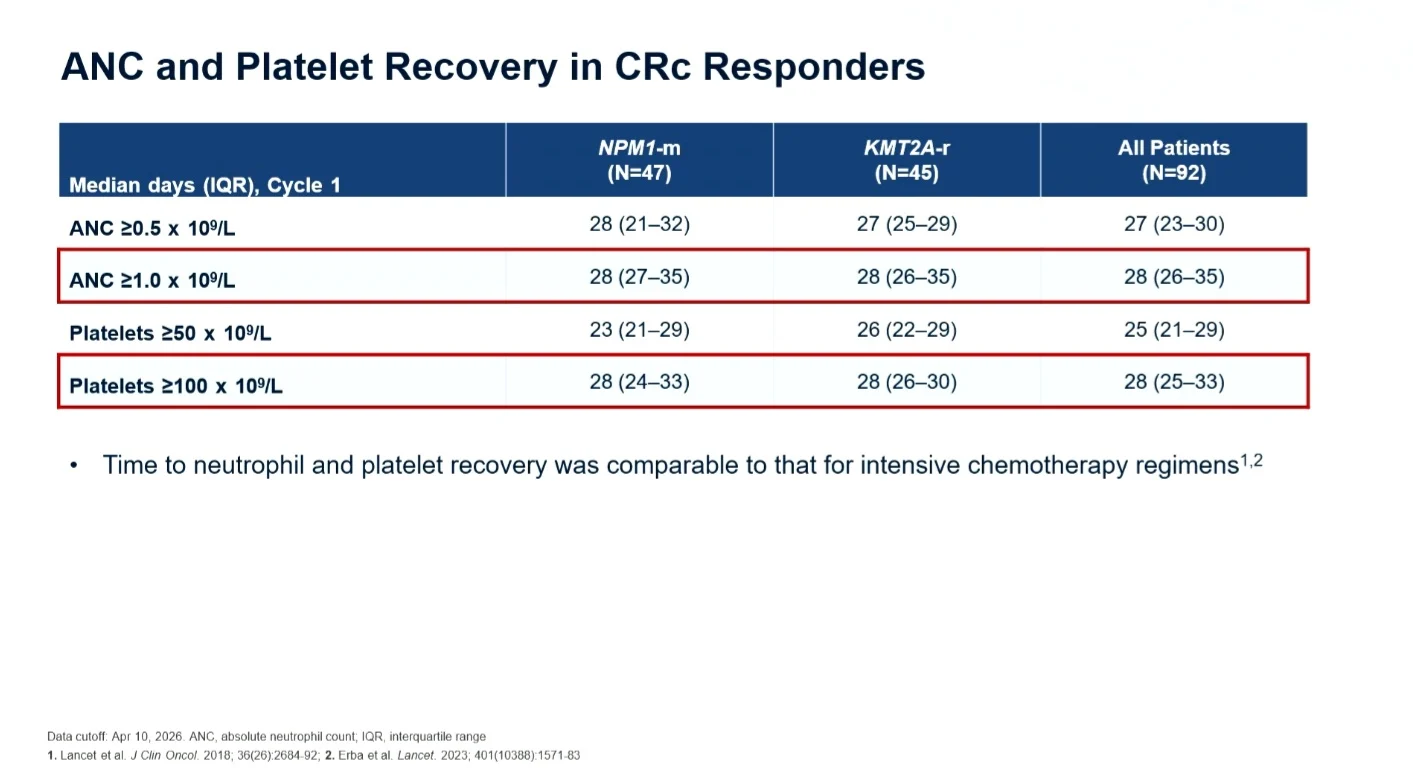
Neutrophil and platelet recovery occurred within expected timeframes for intensive induction therapy, supporting the observation of minimal additive myelosuppression with continuous ziftomenib administration.

Response Rates and MRD Clearance
Ziftomenib demonstrated substantial activity in both molecular subgroups:
- NPM1-mutated AML- CRc rate 96%, ORR 98%
- KMT2A-rearranged AML- CRc rate 90%, ORR 92%
Most responses represented complete remissions, reflecting the depth of clinical activity achieved with the combination.
High remission rates were accompanied by deep molecular responses. Local MRD negativity was achieved in 85% of evaluable responders with NPM1-mutated AML and 82% in KMT2A-rearranged AML.
Central molecular assessment in NPM1-mutated AML confirmed these findings, showing high rates of MRD clearance even at stringent sensitivity thresholds. Molecular responses occurred rapidly, with most patients achieving MRD negativity within the first two treatment cycles.

Response Durability and Survival
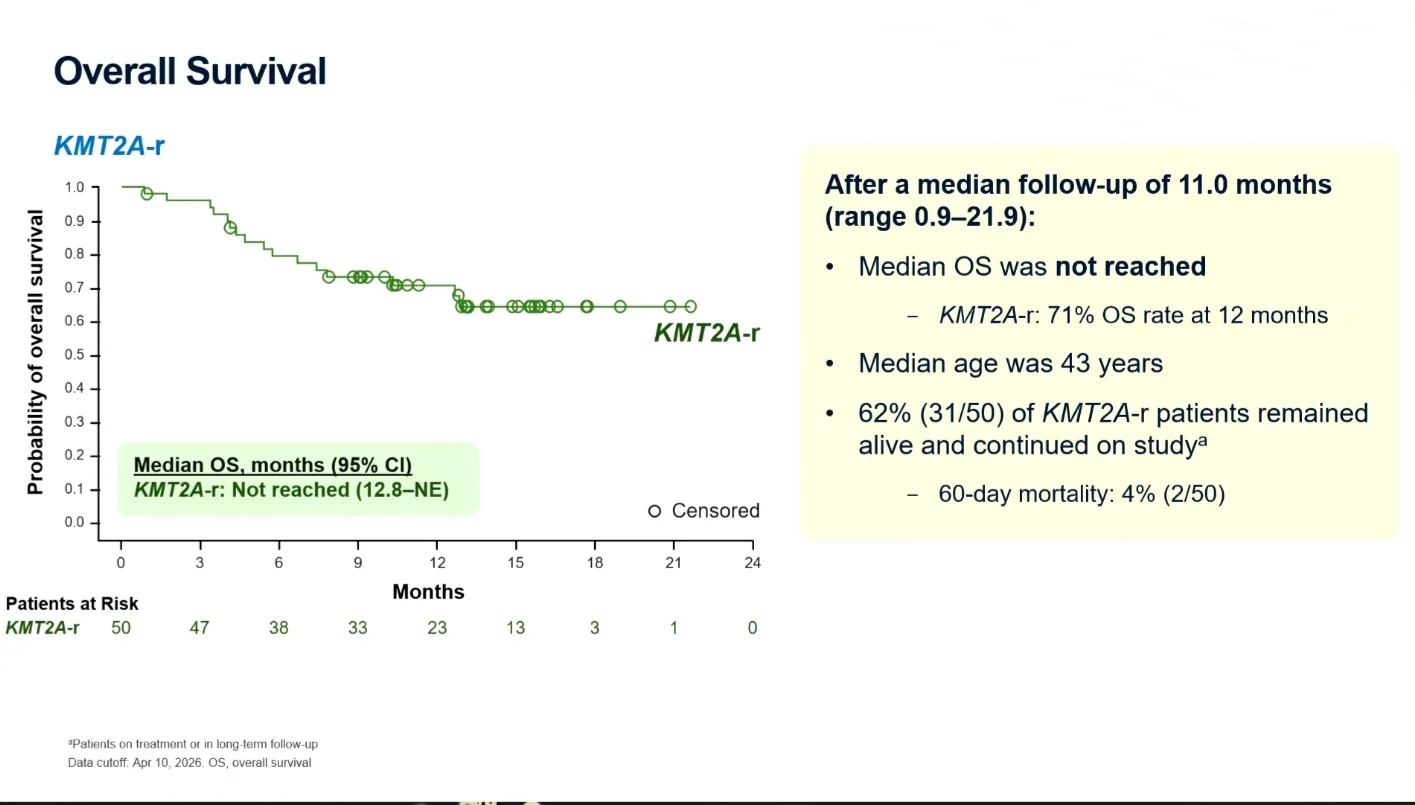
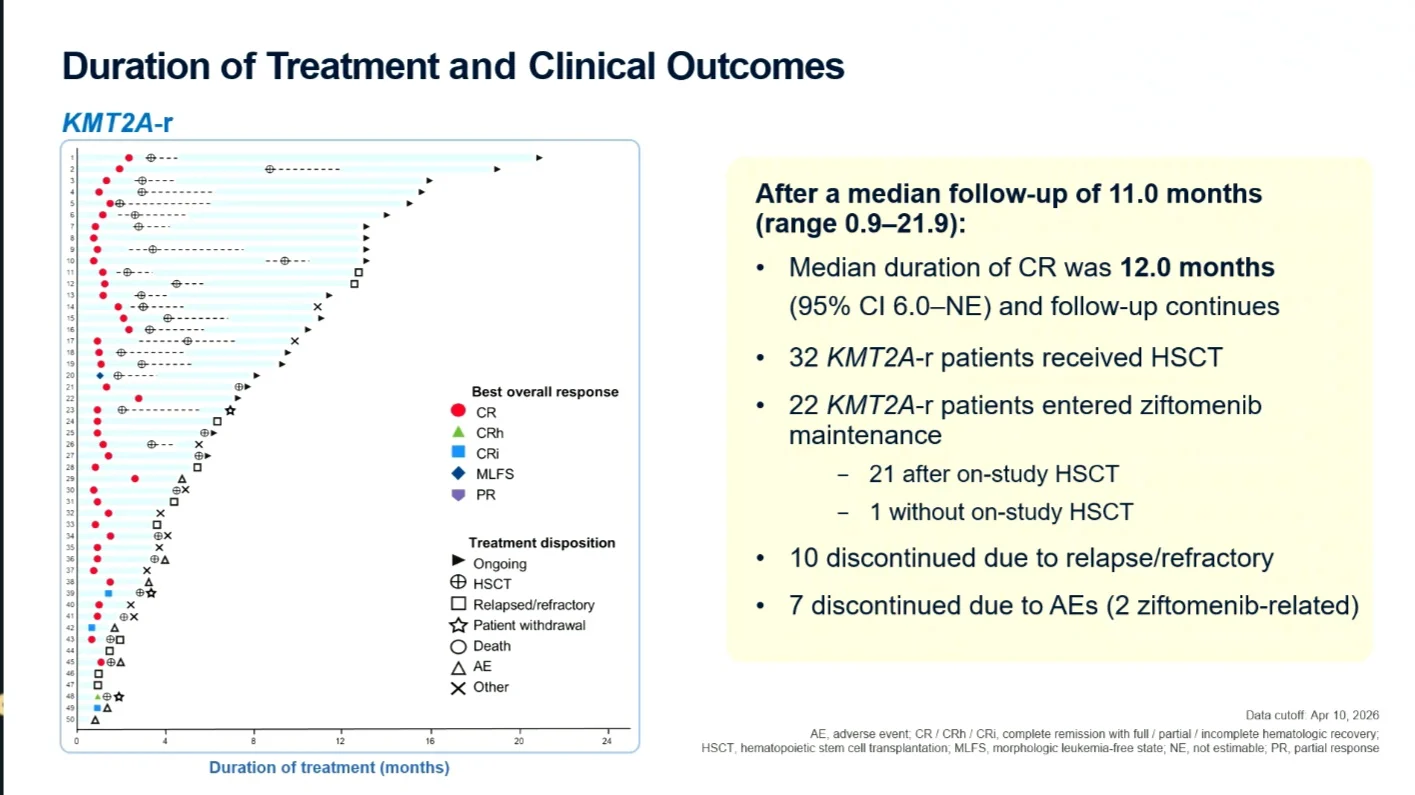
NPM1-mutated AML appeared to achieve slightly deeper and more durable responses. In this cohort, median duration of complete remission had not been reached, with approximately 80% of patients remaining in remission at 12 months. In the KMT2A-rearranged cohort, median CR duration was 12 months, with ongoing follow-up.
Many patients proceeded to HSCT or entered ziftomenib maintenance following induction and consolidation, allowing continued menin inhibition across multiple phases.
Median overall survival was not reached in either cohort at the time of analysis. In NPM1-mutated AML, the estimated 12-month OS rate was 94%, the corresponding rate in the KMT2A-rearranged cohort was 71%. Early mortality remained low, and a substantial proportion of patients continued on study at data cutoff.

Conclusions and Future Perspectives
The updated KOMET-007 results demonstrate that ziftomenib can be effectively combined with intensive frontline chemotherapy, producing high remission rates, deep MRD responses, and durable clinical benefit in both NPM1-mutated and KMT2A-rearranged AML
The combination was generally well tolerated, with manageable differentiation syndrome, infrequent QTc prolongation, and no evidence of clinically meaningful additive myelosuppression. Importantly, treatment could be continued through consolidation, maintenance, and post-transplant settings without the emergence of unexpected toxicities.
As the field increasingly moves beyond morphologic remission toward molecular endpoints, these results provide strong support for the ongoing phase 3 KOMET-017 studies. These two independently powered, registration-enabling, randomized trials are evaluating ziftomenib in both intensive and non-intensive frontline treatment settings in patients with newly diagnosed AML.

{kind=link}
{kind=link}
{kind=link}
{kind=link}