


The growing success of T-cell-redirecting therapies in earlier lines of multiple myeloma has reinforced the notion that patients may derive greater benefit from immune-based therapies before cumulative treatment exposure, immune dysfunction, and clonal evolution diminish therapeutic efficacy.
Presented at the EHA 2026 Plenary Session by Peter Voorhees, MonumenTAL-3 builds on this momentum by evaluating whether talquetamab-based combinations can improve outcomes when introduced earlier in the treatment course of patients with relapsed/refractory multiple myeloma.
Combining GPRC5D Targeting With Immune Modulation
Talquetamab is a first-in-class GPRC5D×CD3 bispecific antibody that has demonstrated deep and durable responses in heavily pretreated RRMM, with long-term follow-up showing sustained disease control. Unlike BCMA-directed therapies, GPRC5D targeting largely spares normal B-cell populations, providing a favorable platform for combination approaches.
Preclinical and clinical data support a complementary interaction between talquetamab, daratumumab, and pomalidomide. Daratumumab not only exerts direct anti-myeloma effects but also reshapes the immune microenvironment by depleting immunosuppressive CD38-positive regulatory cells and promoting recovery of effector T-cell function. Pomalidomide further enhances T-cell and NK cell activity, cytokine production, and reduces T-reg mediated suppression.
This strategy was also supported by results from the phase 1b TRIMM-2, where both Tal-D and Tal-DP produced high response rates and durable clinical activity in heavily pretreated RRMM.

Trial Overview
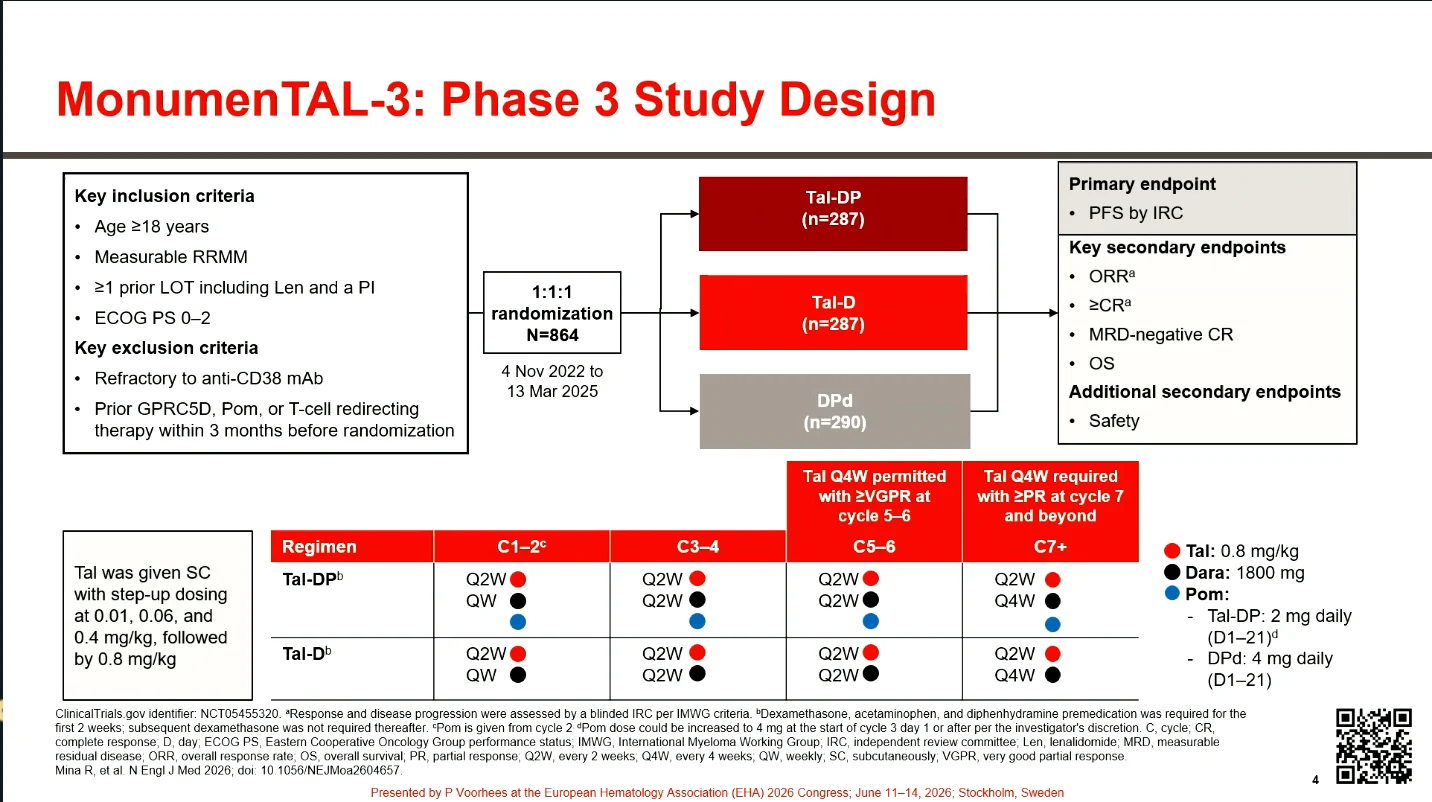
MonumenTAL-3, a global, phase 3 trial was designed to evaluate talquetamab-based combinations in RRMM after at least one prior LOT, including lenalidomide and a proteasome inhibitor. Patients were randomized 1:1:1 to receive Tal-DP, Tal-D, or DPd.
The dual primary comparisons assessed progression-free survival by independent review committee. Key secondary endpoints included ORR, ≥CR, MRD-negative ≥CR at 10⁻⁵ by next-generation sequencing, OS, and safety.
At the time of the preplanned interim analysis, median follow-up was 24.6 months. Approximately 70% of patients in both talquetamab-containing arms remained on study treatment, compared with 47.3% in the DPd arm.
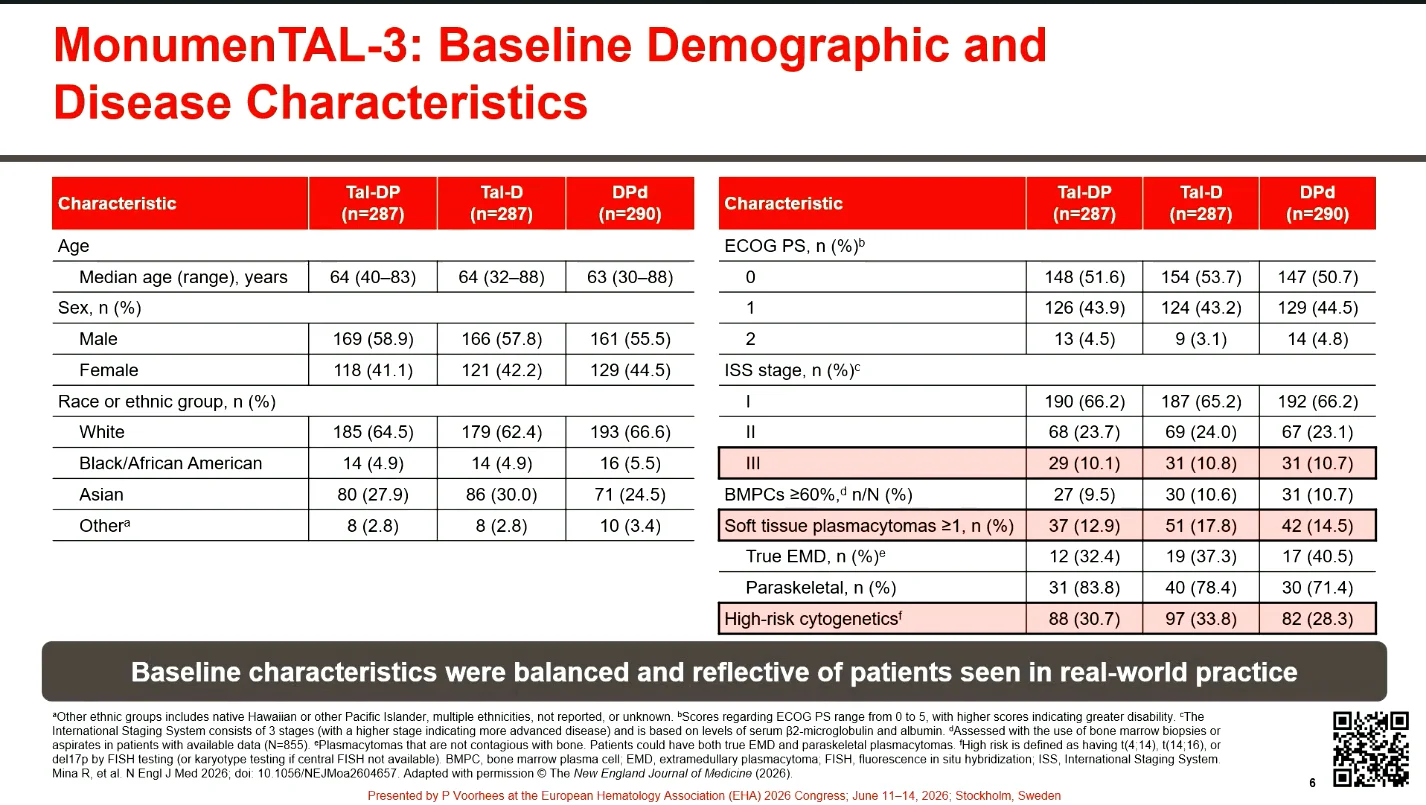
Baseline Characteristics
The median age was approximately 64 years, and most patients had good performance status. High-risk disease features, including adverse cytogenetics and extramedullary disease, were present in a substantial proportion of participants.
Patients had received a median of two prior lines of therapy, while more than 1/3 had received only a single prior regimen. Most patients were refractory to their most recent treatment. All had prior exposure to lenalidomide and a proteasome inhibitor, consistent with the study eligibility criteria, whereas prior anti-CD38 exposure was relatively uncommon. Prior autologous stem cell transplantation had been performed in the majority of patients.

Progression-Free Survival
Both talquetamab-based regimens met the primary endpoint, demonstrating a significant improvement in PFS compared with DPd. At a median follow-up of 24.6 months, median PFS was not reached in either the Tal-DP or Tal-D arm, whereas median PFS was 24.4 months with DPd. The magnitude was substantial, with a 72% reduction in the risk of progression or death for Tal-DP (HR 0.28) and a 67% reduction for Tal-D (HR 0.33) versus DPd.

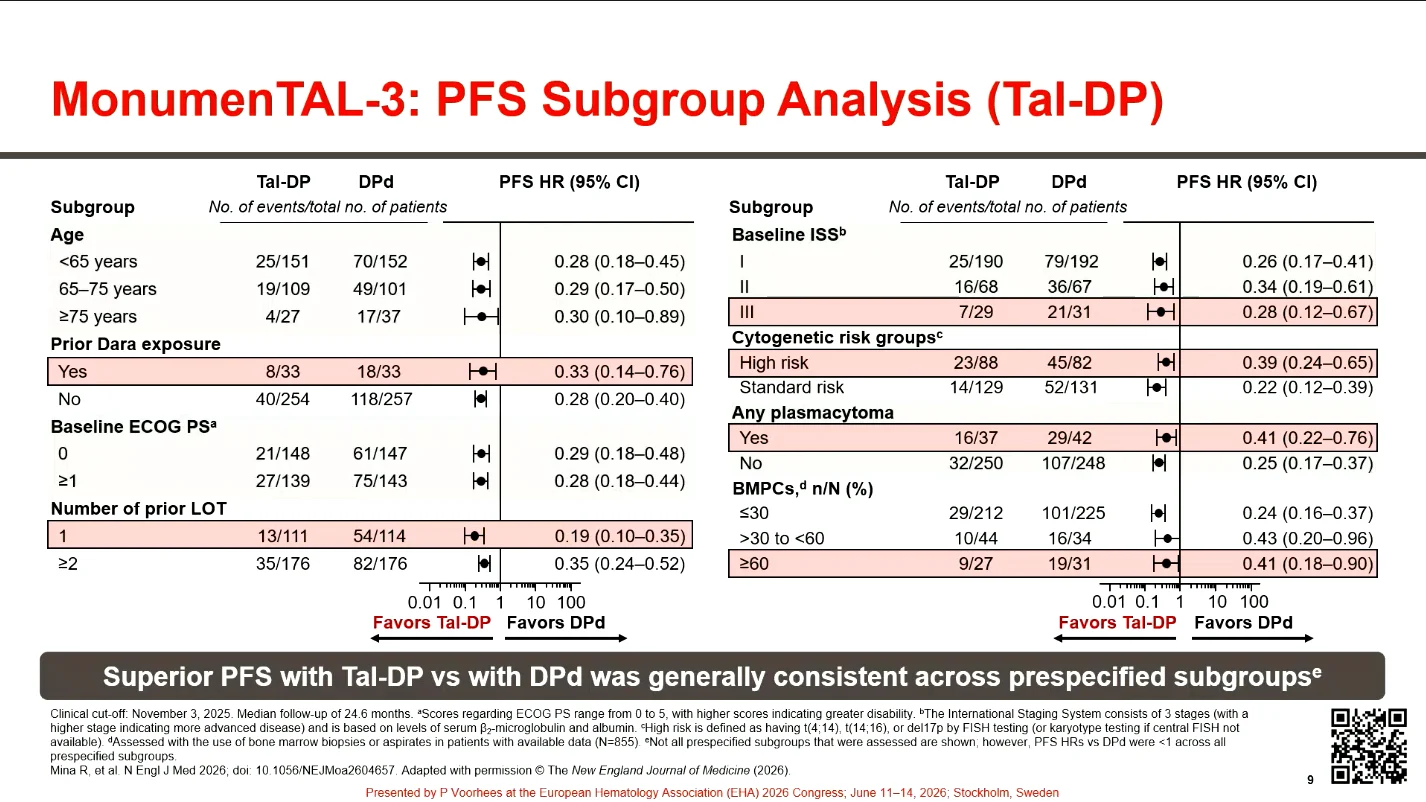
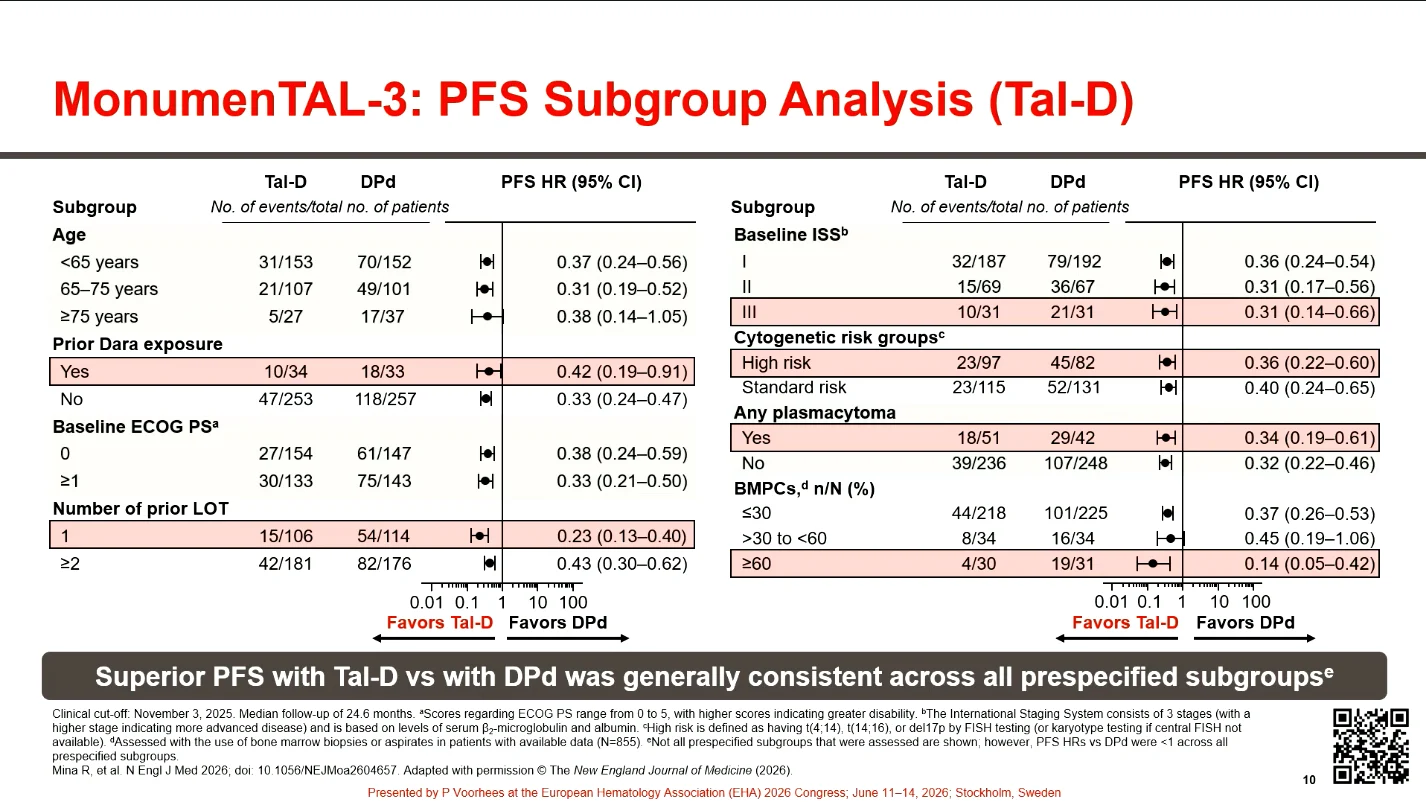
PFS Across Subgroups
The PFS benefit was consistent across prespecified patient subgroups, including those defined by age, performance status, disease stage, cytogenetic risk, plasmacytoma status, and prior anti-CD38 exposure. Both talquetamab-containing regimens maintained activity in patients with high-risk cytogenetics and extramedullary disease. The greatest relative benefit was observed in patients treated after only one prior LOT, supporting the value of introducing T-cell-redirection earlier in the course.
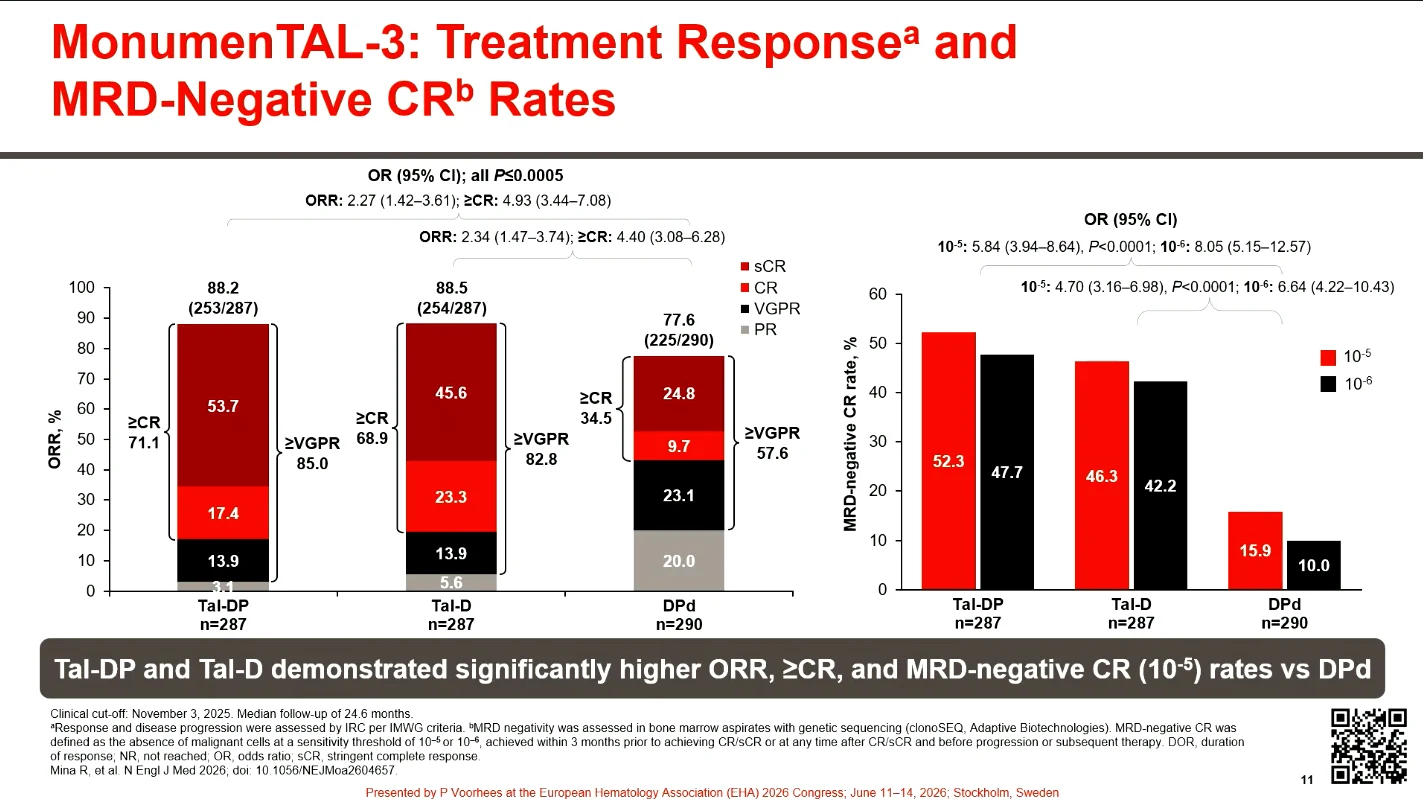
Response and MRD Negativity
Responses were deeper and more frequent with both talquetamab-based combinations. ORR exceeded 88% in both experimental arms, accompanied by substantially higher rates of ≥CR and MRD-negative CR. More than half of patients receiving Tal-DP and nearly half receiving Tal-D achieved MRD-negative CR at the 10⁻⁵ threshold, compared with a markedly lower rate in the DPd arm.
Overall Survival
An early OS advantage was observed for both talquetamab-containing regimens. At 24 months, more than 87% of patients treated with Tal-DP or Tal-D remained alive, compared with 79% of those receiving DPd. Though the prespecified boundary for OS superiority had not yet been crossed at the time of this interim analysis, both comparisons demonstrated a clinically meaningful reduction in the risk of death.

Safety in Focus
The overall safety profile of both talquetamab-based regimens was consistent with the known toxicities of their individual components and did not reveal new safety signals. Rates of treatment discontinuation due to TEAEs were low across all arms, and TEAE-related deaths were uncommon.

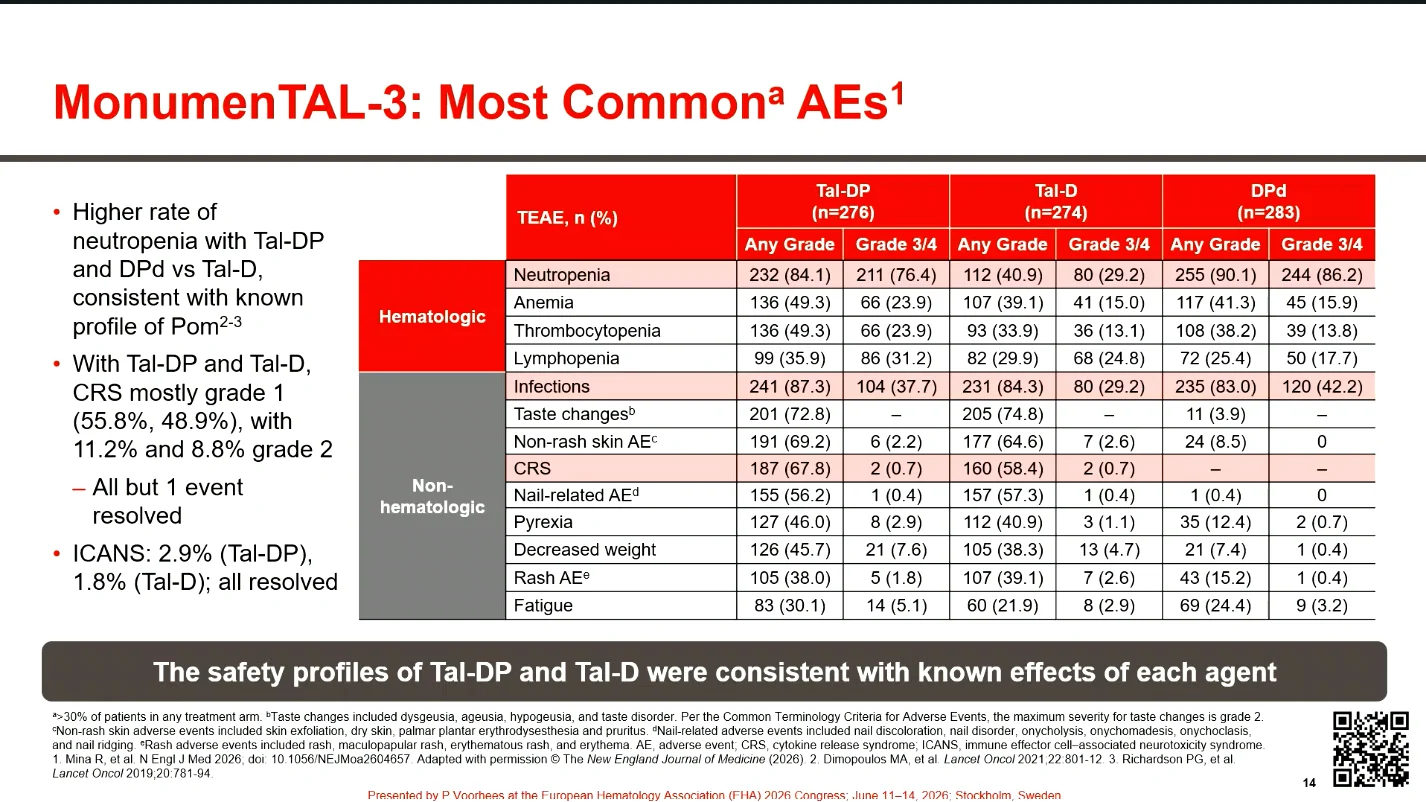
Adverse Events
Hematologic toxicities were among the most common AEs. As expected, neutropenia occurred more frequently with Tal-DP and DPd than with Tal-D, consistent with the inclusion of pomalidomide. Common nonhematologic AEs associated with talquetamab included taste changes, skin and nail toxicities, pyrexia, and weight loss.
Taste, skin, and nail toxicities are believed to be related to GPRC5D expression in normal tissues. Early nutritional monitoring and supportive care are important particularly in patients experiencing dysgeusia and weight loss.
CRS was frequent but predominantly low grade, with most events limited to grade 1 or 2 and nearly all resolving. ICANS was infrequent in both talquetamab-containing arms, and all reported cases resolved.

Infections
Infections were common across treatment groups, reflecting the heavily immunocompromised nature of the study population. Importantly, rates of grade 3-4 infections were numerically lower with Tal-D and comparable between Tal-DP and DPd. Severe infections occurred most often during the first six months of therapy and declined thereafter. Fatal infections were uncommon across all treatment arms.
Hypogammaglobulinemia
Hypogammaglobulinemia was more frequent in the talquetamab-containing arms than with DPd, consistent with prolonged immune-directed therapy. Opportunistic infections were reported in a minority of patients, without new infectious safety concerns.
Talquetamab-Based Therapy in 2L and Beyond for RRMM
MonumenTAL-3 demonstrated that talquetamab-based combinations significantly improved PFS vs DPd, with consistency across relevant subgroups and improvements in OS. High rates of ≥CR and MRD-negative CR further supported the efficacy of both combinations.
The safety profiles were consistent with the known effects of their individual components. Talquetamab was readily combinable with daratumumab, with low rates of treatment discontinuation due to AEs. Tal-D was associated with a favorable infection profile, while higher rates of cytopenias with Tal-DP were consistent with the addition of pomalidomide.
Though efficacy outcomes numerically favored Tal-DP over Tal-D, both regimens demonstrated substantial clinical benefit. These findings support Tal-D, with or without pomalidomide, as a new standard-of-care option for patients with RRMM beginning as early as 2L across diverse clinical practice settings.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}