


Initial results from the phase 3 SUCCESSOR-2 trial (NCT05552976), the first randomized study evaluating mezigdomide in RRMM, comparing MeziKd versus Kd, were presented by Paul G. Richardson, MD, at ASCO 2026.
MeziKd showed a clinically meaningful PFS benefit as early as first relapse in a predominantly triple-class-exposed population with significant unmet need.
Background
Treatment sequencing in RRMM is becoming more complex as increasing numbers of patients entering second-line therapy are already lenalidomide- and anti-CD38 monoclonal antibody-exposed, limiting subsequent treatment options.
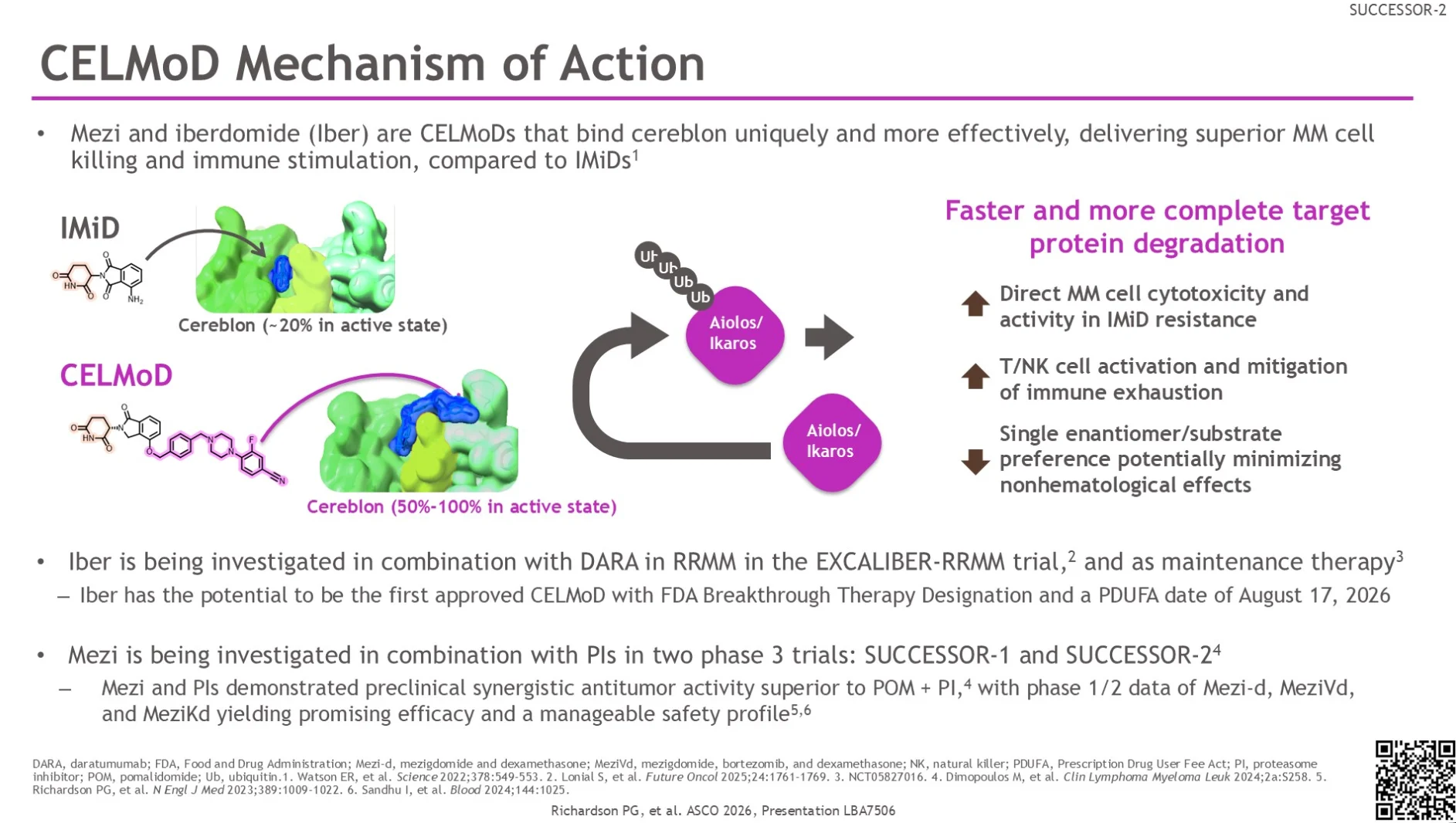
Mezigdomide (Mezi) is an investigational oral cereblon E3 ligase modulator (CELMoD) designed to induce potent degradation of the transcription factors Ikaros and Aiolos. Compared with currently available IMiDs, mezigdomide demonstrates enhanced immune activation and more potent anti-myeloma activity in preclinical studies.
Study Design
This randomized, two-stage, inferentially seamless phase 3 trial enrolled patients with RRMM who had received at least one prior line of therapy, including both lenalidomide and an anti-CD38 MoAb .
In stage 1, patients were randomized in a 3:3:3:2 ratio to receive mezigdomide at doses of 0.3 mg, 0.6 mg, or 1.0 mg in combination with carfilzomib-dexamethasone, or Kd alone, with the goal of selecting the optimal mezigdomide dose for stage 2. The selected dose was 1.0 mg.
In stage 2, patients were randomized 3:2 to receive MeziKd or Kd. Mezigdomide was administered on days 1-21 of 28-day cycles. Carfilzomib was given weekly at 56 mg/m² with weekly dexamethasone in the MeziKd arm. The control arm received either twice-weekly carfilzomib 56 mg/m² or weekly carfilzomib 70 mg/m² plus dexamethasone.
The primary endpoint was PFS. Secondary endpoints included ORR, OS, safety and dose selection.

Enrolled Population
A total of 479 patients were included in the analysis, including 288 patients treated with MeziKd at the selected 1.0 mg dose and 191 patients treated with Kd alone.
The study population reflected a heavily pretreated and high-risk RRMM cohort:
- Median age was 68 years (30-85), and 25.1% of patients were aged 75 years or older.
- Median number of prior LOTs was 2 (1-9).
- 92.1% of patients were triple-class exposed, 85.8% were refractory to anti-CD38 therapy, 75.8% were Len-refractory.
- Prior pomalidomide exposure was reported in 37.2% of patients, 7.3% had received prior anti-BCMA therapy.
Efficacy Findings
At a median follow-up of 10.6 months, treatment exposure favored the investigational arm, with 52.4% of patients remaining on MeziKd vs 31.4% on Kd. Median treatment duration was longer with MeziKd (8.9 months) vs Kd (6.2 months).

Median PFS was 18.0 months (95% CI, 14.5-22.1) with MeziKd compared with 8.3 months (95% CI, 5.6-10.7) with Kd alone, corresponding to a 52% reduction in the risk of progression or death.
The PFS benefit was consistent across clinically important subgroups, including patients with more than two prior lines of therapy, high-risk cytogenetics, extramedullary disease, prior treatment refractoriness and patients aged ≥75 years.
Response outcomes also favored MeziKd:
- The OS rate reached 80.2% vs 53.4% in the Kd arm.
- CR or better rates were 26.7% vs 8.9%
- Death rates were 21.5% vs 26.7%
Safety Data
Grade 3-4 treatment-emergent AEs were more frequent with MeziKd (83.7% vs 56.5%).
1. Neutropenia occurred in 61.1% vs 9.1% of patients.
2. Grade 3-4 infections were reported in 34.0% vs 15.6%.
3. Grade 5 infections remained infrequent in both arms (2.4% vs 1.1%).
The safety profile appeared predictable and clinically manageable.

Clinical Takeaway
SUCCESSOR-2 is the first phase 3 trial demonstrating clinically meaningful benefit with mezigdomide in RRMM. Mezigdomide plus Kd nearly doubled median PFS compared with Kd alone (18.0 vs 8.3 months) and achieved higher response depth, including a threefold increase in CR or better rates.
The trial enrolled a predominantly triple-class-exposed and refractory RRMM population. Clinical benefit was consistent across difficult-to-treat subgroups: elderly patients, high-risk cytogenetics, and extramedullary disease. Increased neutropenia and infections were observed with MeziKd, but severe infectious mortality remained low.
These findings support MeziKd as a potential new standard-of-care option across various RRMM settings.
Contextualization Across RRMM Clinical Trials
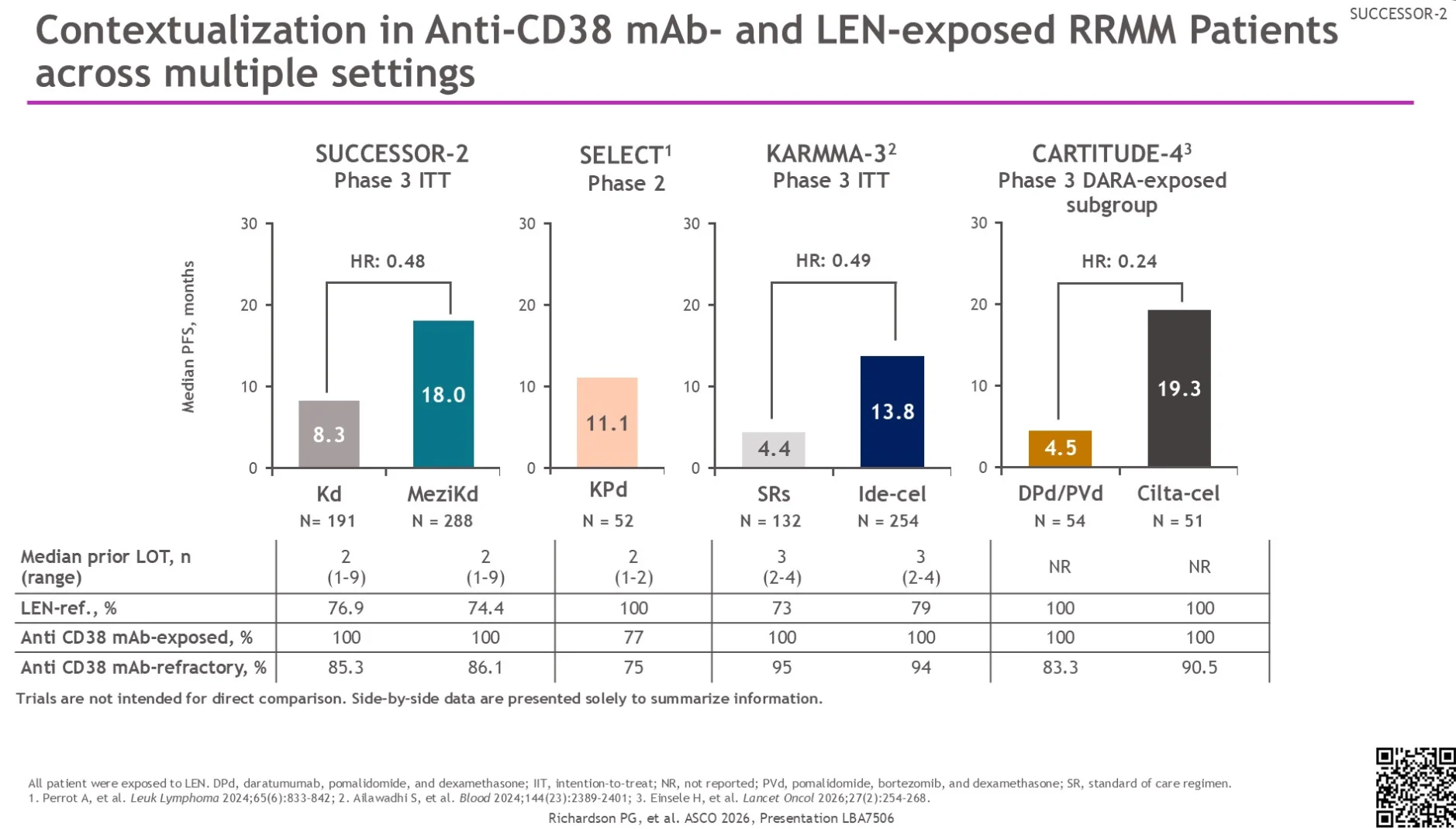
The efficacy observed with MeziKd in SUCESSOR-2 provides important context alongside outcomes reported in other anti-CD38 monoclonal antibody- and lenalidomide-exposed RRMM studies across different treatment modalities.
For contextual reference, SELECT (phase 2) reported a median PFS of 11.1 months with KPd. In KARMA-3, median PFS was 13.8 months with ide-cel versus 4.4 months with standard regimens (HR 0.49). In the CARTITUDE-4 phase 3 daratumumab-exposed subgroup, cilta-cel achieved a median PFS of 19.3 months versus 4.5 months with DPd/PVd (HR 0.24).
Although cross-trial comparisons should be interpreted cautiously, findings support the potential role of oral MeziKd as an effective and accessible treatment option, including in community practice.
Follow More Trial Updates From ASCO 2026 With OncoDaily.
{kind=link}
{kind=link}