


Among the recurring themes at EHA 2026 was the growing focus on biologically driven therapies. In myelofibrosis, one of the most anticipated presentations was the phase 1 evaluation of INCA033989, a first-in-class mutant calreticulin-targeted monoclonal antibody. The data were presented by Claire Harrison, who was also honored with the 2026 EHA Lifetime Achievement Award.

From Downstream Signaling to Clone-Directed Therapy
Myelofibrosis is a chronic myeloproliferative neoplasm characterized by bone marrow fibrosis, splenomegaly, anemia, and debilitating symptoms. JAK inhibitors have become the cornerstone of MF treatment, but they primarily address downstream signaling and the clinical manifestations of disease while having limited impact on the malignant clone responsible for disease initiation and maintenance.
Mutations in exon 9 of the calreticulin (CALR) gene occur in approximately 25-35% of patients with MF and represent a major disease-driving event. Current therapies are not mutation-specific. INCA033989 is a novel, fully human, Fc-silenced IgG1 monoclonal antibody that selectively targets mutant CALR in complex with the thrombopoietin receptor (TPO-R), thereby inhibiting oncogenic signaling and cellular proliferation.
Study Design and Patient Population
INCA033989 is being evaluated in the ongoing phase 1 INCA033989-101 and INCA033989-102 studies in patients with MF or ET. This analysis included adults with CALR-mutated primary or post-ET MF. Patients received INCA033989 either as:
- Monotherapy, if they were relapsed, refractory, intolerant to, or ineligible for JAK inhibitor therapy.
- Combination therapy with ruxolitinib, if they had received at least 12 weeks of ruxolitinib but had a suboptimal response.
The primary endpoints were safety and tolerability. Secondary endpoints included spleen volume reduction (SVR25 and SVR35), anemia response, symptom improvement assessed by MPN-SAF Total Symptom Score, and changes in mutant CALR allele burden.
Seventy patients with CALR-mutated MF were included in the analysis. Most patients had intermediate-risk disease, substantial splenomegaly, symptomatic burden, and baseline anemia. Type 1 CALR mutations accounted for 59% of cases, while 21% harbored Type 2 mutations and 20% had other CALR variants.
Safety and Tolerability
INCA033989 demonstrated a favorable safety profile both as monotherapy and in combination with ruxolitinib.
No dose-limiting toxicities were observed, and a maximum tolerated dose was not reached. At the time of analysis, 84% of patients remained on monotherapy and 76% remained on combination treatment.
Treatment-emergent adverse events were predominantly hematologic and included thrombocytopenia, anemia, and neutropenia. Grade ≥3 events were generally manageable and occurred most frequently in patients with pre-existing cytopenias. Treatment discontinuations and dose reductions due to adverse events were uncommon.

Spleen Responses
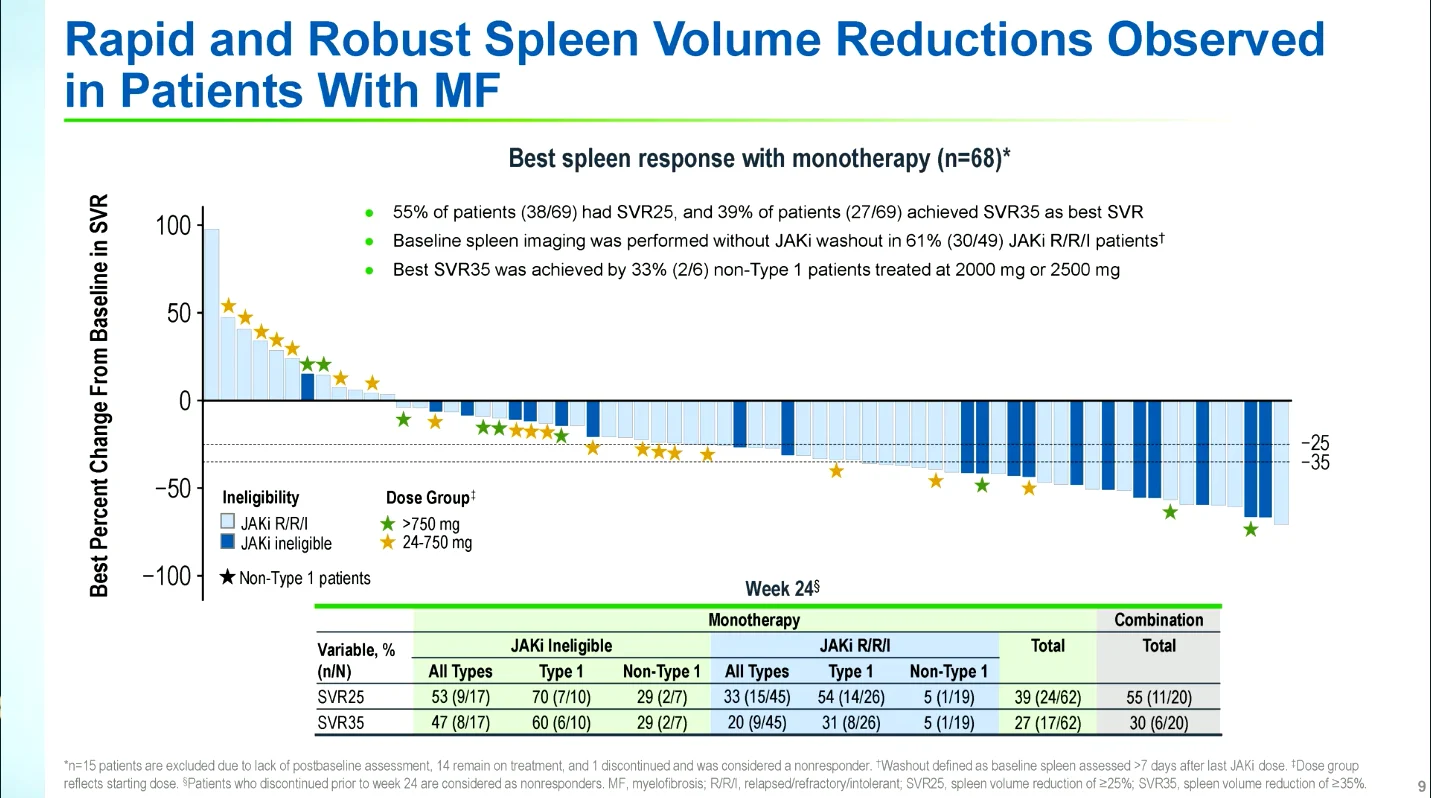
At Week 24, both treatment approaches demonstrated substantial reductions in spleen volume:
- SVR25: 44% with INCA033989 monotherapy vs 63% with combination therapy
- SVR35: 31% with INCA033989 monotherapy vs 38% with combination therapy
Responses were observed across CALR mutation subtypes in both JAK inhibitor-naïve and previously treated patients.
Symptom and Anemia Improvement
At Week 24, approximately one-third of evaluable patients achieved a 50% reduction in total symptom score (TSS50) in both monotherapy and combination cohorts.
Anemia improvement represented one of the most notable findings of the study. Among evaluable patients receiving monotherapy, 58% achieved an anemia response, including major responses in more than half of patients. Improvements in hemoglobin were observed in both JAKi-ineligible patients and those who were relapsed, refractory, or intolerant to prior JAKi. Anemia responses were also observed in patients receiving INCA033989 plus ruxolitinib.

Molecular and Cellular Effects
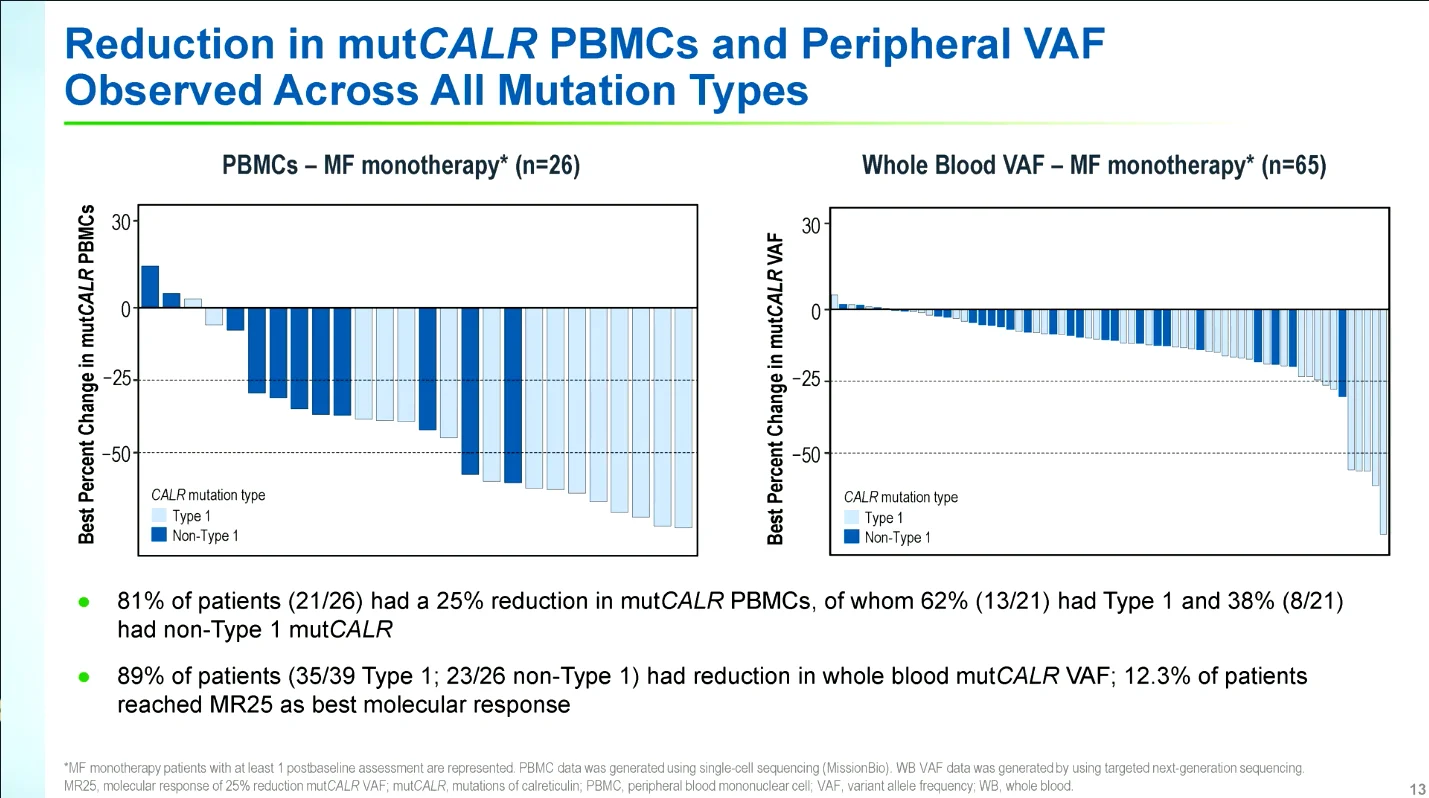
Consistent reductions in mutant CALR burden were observed. Among evaluable patients receiving monotherapy:
- 91% experienced a reduction in CALR variant allele frequency (VAF)
- 81% achieved at least a 25% reduction in mutCALR-positive peripheral blood mononuclear cells
- 89% demonstrated reductions in whole-blood mutCALR VAF
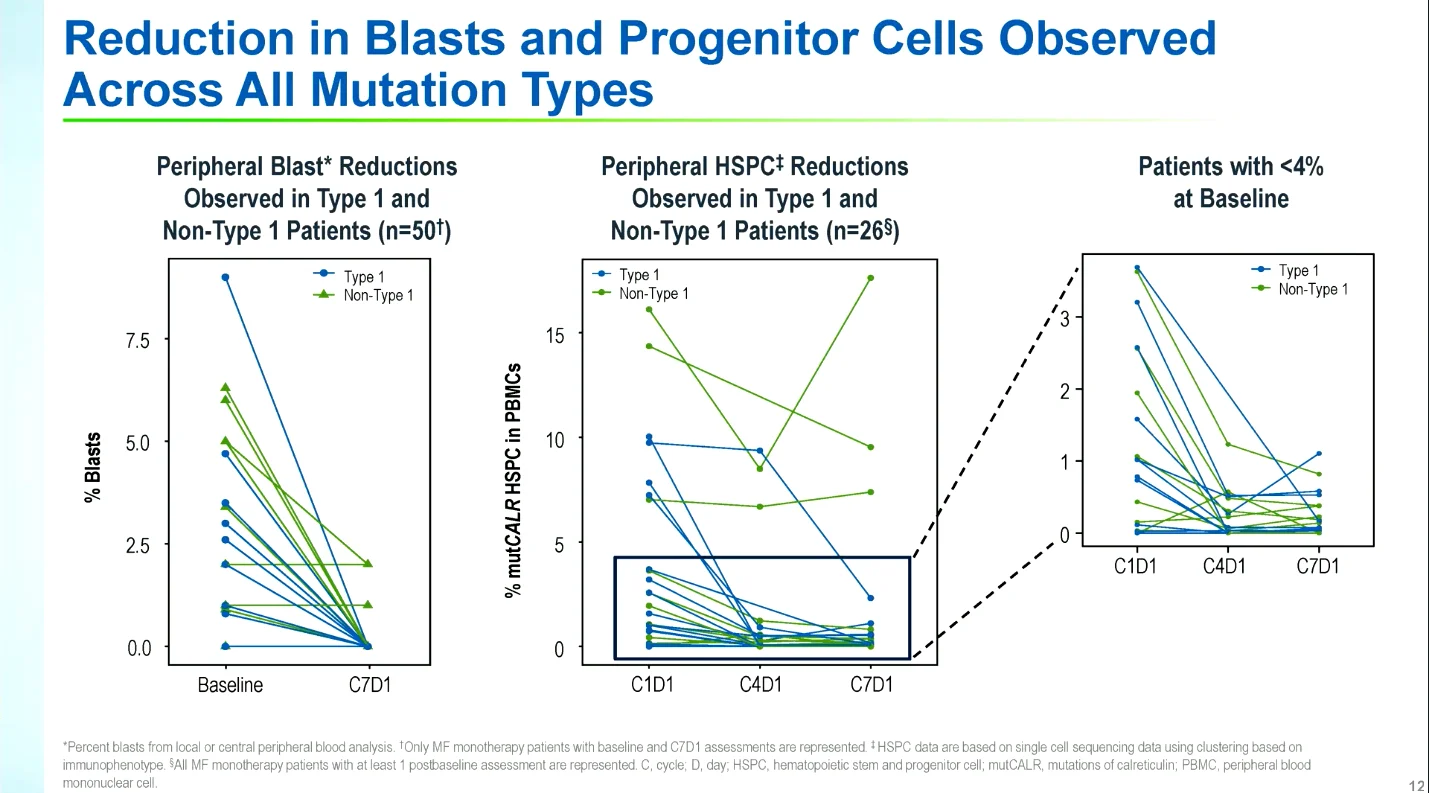
Importantly, reductions were observed across both Type 1 and non-Type 1 CALR mutations. Treatment was also associated with decreases in circulating blasts and mutant CALR-positive hematopoietic stem and progenitor cells, disease-sustaining cellular populations.
Bone Marrow Findings and Disease Modification
Treatment reduced mutant CALR-positive megakaryocyte populations and was associated with improvement or stabilization of bone marrow fibrosis. Among evaluable patients with paired assessments, 40% demonstrated improvement in fibrosis grade, while the remainder maintained stable disease.

Key Takeaways
INCA033989 demonstrated favorable tolerability and meaningful clinical activity in patients with CALR-mutated myelofibrosis who were relapsed, refractory, intolerant to, or ineligible for JAK inhibitor therapy, as well as in patients with a suboptimal response to ruxolitinib.
Robust spleen, symptom, and anemia responses were accompanied by reductions in mutant CALR allele burden, decreases in blasts and progenitor-cell populations, and improvements in bone marrow pathology. Collectively, these findings suggest that INCA033989 may exert effects beyond symptomatic disease control.
These results support the ongoing phase 3 development of INCA033989 in patients with CALR-mutated myelofibrosis.

Myelofibrosis (MF) in 2026: Matching Therapy to the Dominant Clinical Problem
{kind=link}
{kind=link}
{kind=link}