


During the EHA 2026 Plenary Session, Martin Schrappe presented results from the randomized high-risk arm of the AIEOP-BFM ALL 2017 trial, assessing the replacement of two intensive chemotherapy blocks with two cycles of blinatumomab in children with newly diagnosed high-risk B-cell acute lymphoblastic leukemia (B-ALL).
Background
In pediatric high-risk B-ALL, treatment intensification is often required because of adverse biologic features or persistent MRD. While effective, intensive chemotherapy blocks contribute substantially to infectious complications, organ toxicity, prolonged hospitalization, and treatment-related mortality.
Blinatumomab, a CD19-directed bispecific T-cell engager, has demonstrated potent activity in relapsed/refractory and MRD-positive B-ALL, raising the possibility that selected chemotherapy elements could be replaced by immunotherapy without compromising anti-leukemic efficacy in a population at increased risk of relapse.
You can watch more on OncoDaily TV
Treatment Arms and Objectives
AIEOP-BFM ALL 2017 is an international investigator-initiated, multicenter, open-label phase III trial.
Between 2018 and September 2023, 5,068 patients were enrolled. Among 4,298 patients with B-ALL, 905 met protocol-defined high-risk criteria based on adverse genetic features, high MRD levels, or inadequate early treatment response.
After induction, consolidation, and one intensive chemotherapy block (HR-1′), eligible HR patients underwent randomization. Of 768 eligible patients, 709 were randomized:
- Experimental arm: two 28-day cycles of blinatumomab plus intrathecal methotrexate (n=358).
- Control arm: standard HR-2′ and HR-3′ intensive chemotherapy blocks (n=351).

The primary objective was improvement in EFS of at least 10%. Secondary objectives were relapse incidence, MRD response, treatment-related toxicity, mortality, and outcomes following allogeneic HSCT.
Baseline characteristics were well balanced between groups. More than half of patients fulfilled NCI high-risk criteria, and the cohort was enriched for adverse biological features including hypodiploidy, KMT2A rearrangements, and persistent MRD.

Event-Free Survival
At the planned interim analysis, blinatumomab significantly improved outcomes compared with chemotherapy.
The 4-year EFS was 83.0% in the experimental arm vs 70.3% in the control arm, corresponding to a hazard ratio of 0.51. A total of 46 events occurred in the blinatumomab arm compared with 83 in the chemo arm.
Relapse Incidence
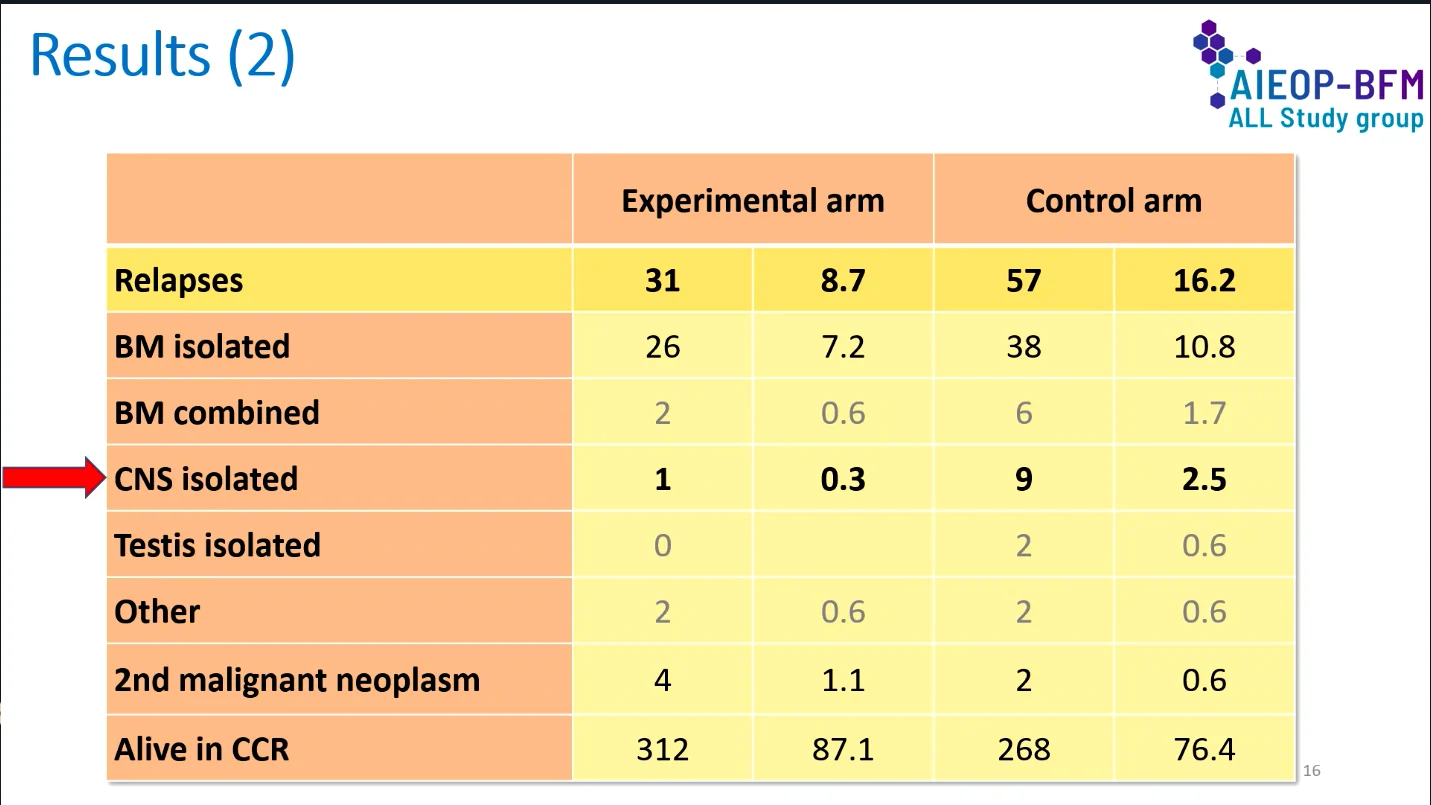
The improvement in EFS was primarily driven by a reduction in relapse.
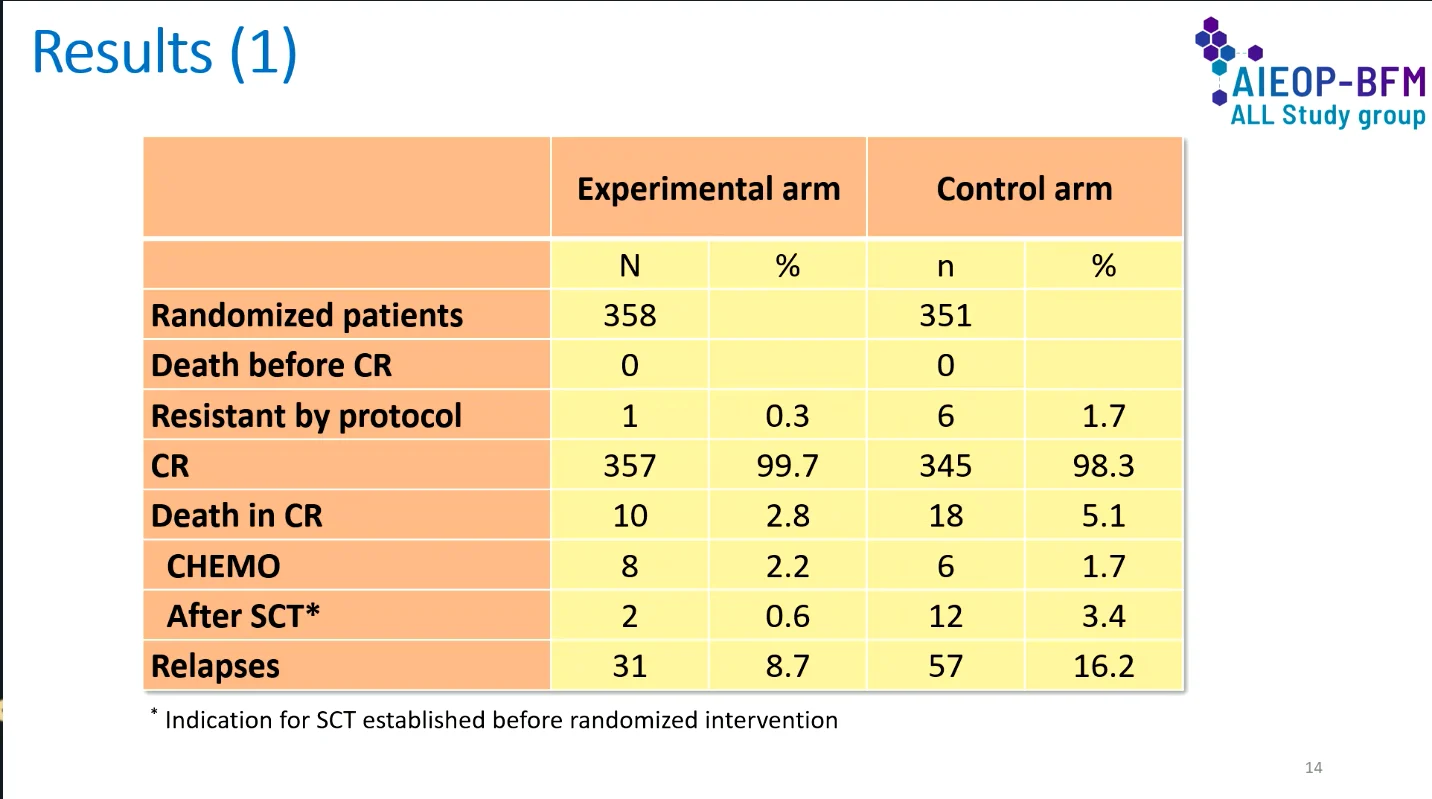
The 4-year cumulative incidence of relapse was 11.8% with experimental arm compared with 21.4% with chemotherapy. Overall, 31 relapses vs 57 in the control arm.
Bone marrow relapse remained the most common relapse type in both groups. Isolated CNS relapse was uncommon with blinatumomab, occurring in only 1 patient vs 9 patients in the chemo arm.
MRD Response
Blinatumomab produced substantially deeper MRD responses than chemotherapy.
Among patients who remained MRD-positive after HR-1′, MRD burden decreased in 76.9% of patients after the first cycle of blinatumomab compared with 45.8% after HR-2′ chemotherapy.
The clinical impact of this response was reflected in subsequent outcomes. Among patients who were MRD-positive before randomization, 4-year EFS was 79.1% with blinatumomab vs 58.3% with chemotherapy. An EFS benefit was also observed in patients who were MRD-negative before randomization.

Remission and Survival
Complete remission rates remained high in both groups, reaching 99.7% with blinatumomab and 98.3% with chemotherapy.
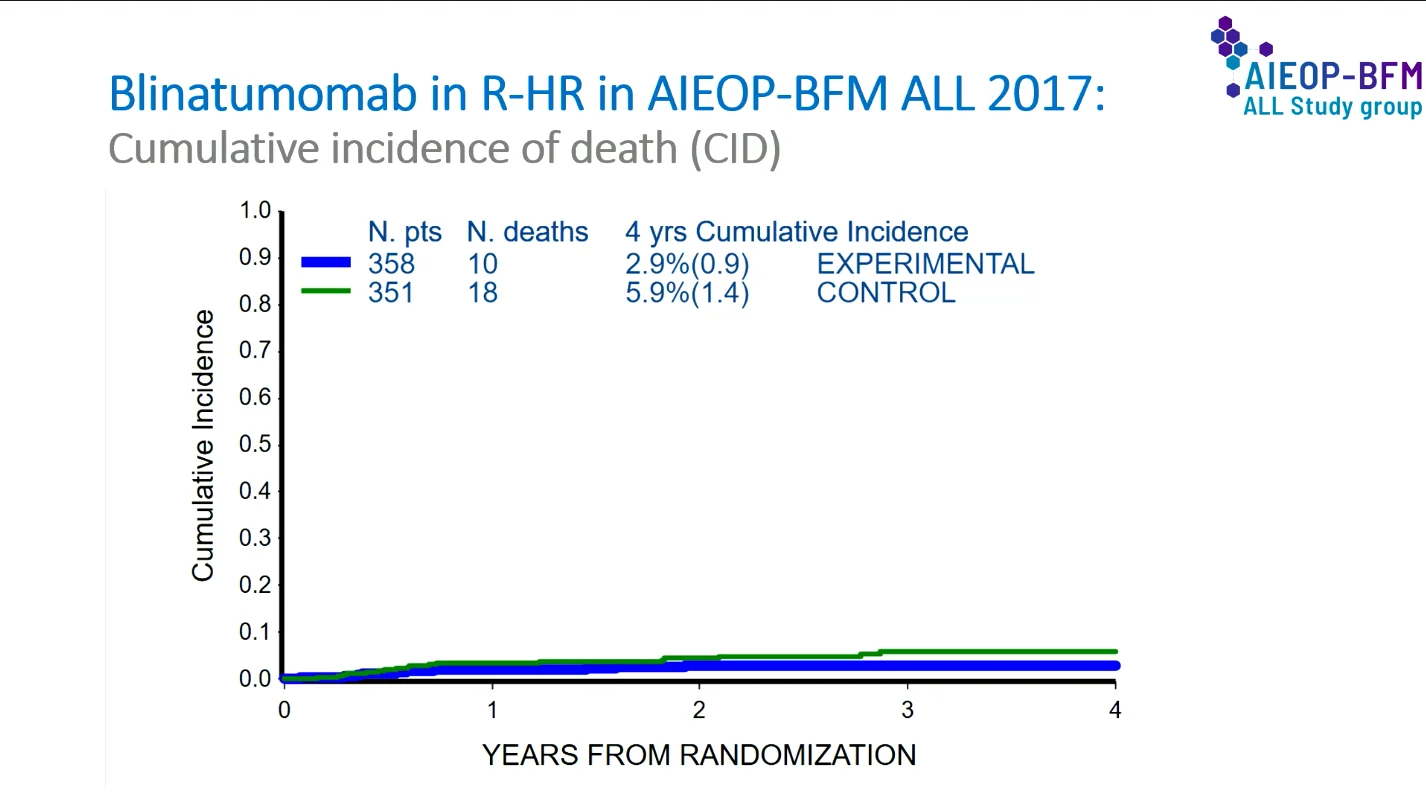
Deaths in complete remission were less frequent in the experimental arm (10 vs 18 patients), resulting in a lower 4-year cumulative incidence of death.
Overall survival numerically favored blinatumomab, with 4-year OS rates of 93.6% and 91.0% in the experimental and control arms, respectively.
A greater proportion of patients remained alive in continuous complete remission in the blinatumomab arm (87.1% vs 76.4%).
Subgroup Analysis
The treatment effect was consistent across most predefined high-risk subgroups, including age, sex, leukocyte count, NCI risk category, genetic risk features, and MRD-defined groups. The forest plot analysis generally favored blinatumomab, supporting the robustness of the observed EFS benefit across the high-risk population.
Safety
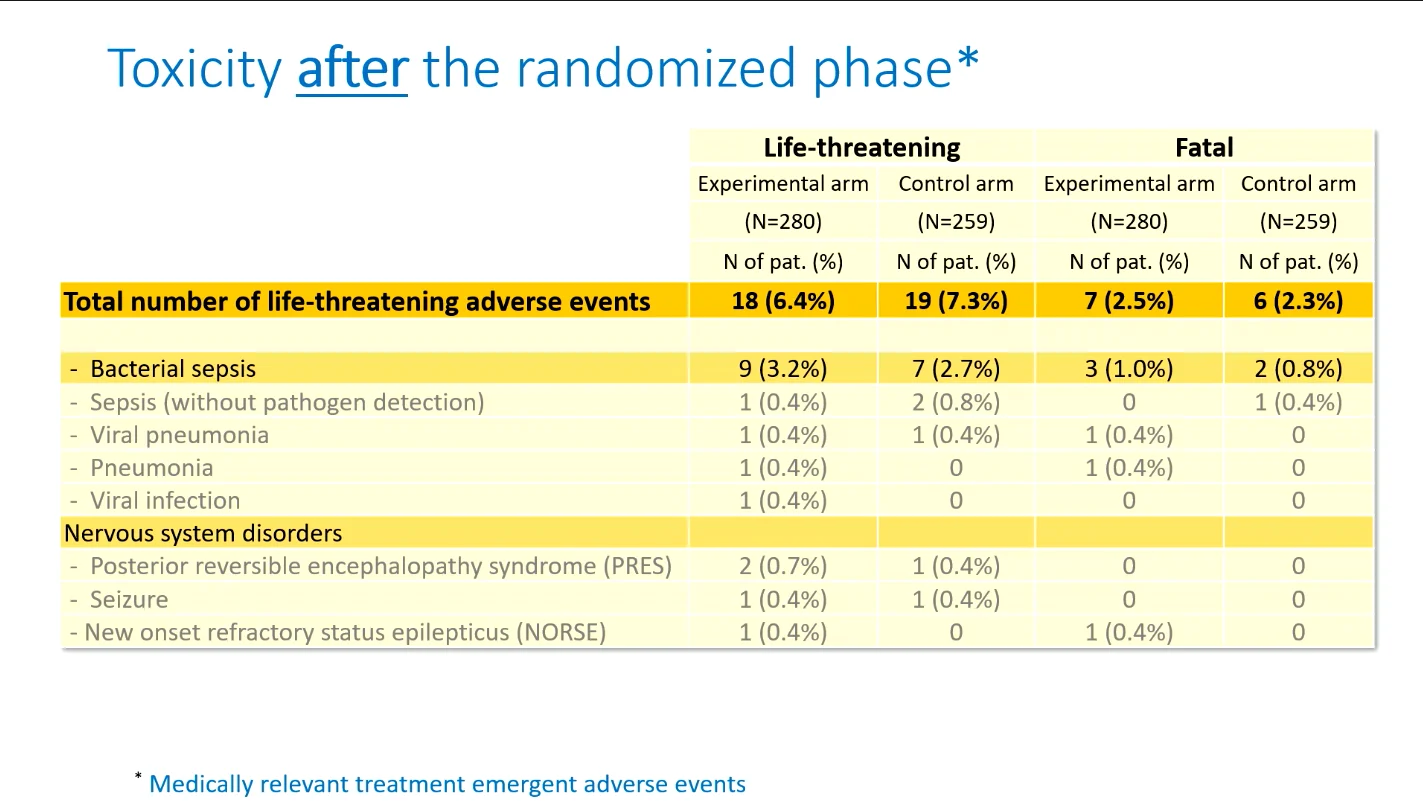
During the randomized treatment phase, blinatumomab substantially reduced several major chemotherapy-associated toxicities.
Clinically relevant infections occurred in 23.9% of patients receiving blinatumomab vs 69.4% of those receiving chemotherapy. Severe mucositis was markedly less frequent with blinatumomab (0.3% vs 10.0%), as were pancreatitis and allergic reactions.
As expected, neurologic adverse events occurred more frequently with blinatumomab (12.0% vs 3.2%). However, severe neurologic complications remained uncommon.
Life-threatening infections during the randomized phase occurred in 11 patients in the chemotherapy arm and in none of the patients receiving blinatumomab.
Among patients proceeding to allogeneic HSCT, non-relapse mortality was substantially lower following blinatumomab-based treatment (2.5% vs 16%).

Conclusion
This strategy improved EFS, reduced relapse risk, deepened MRD responses, and decreased treatment-related toxicity. Although neurologic adverse events require careful monitoring, the overall safety profile favored blinatumomab. For the first time in newly diagnosed ALL, highly toxic chemotherapy elements were successfully replaced by blinatumomab, demonstrating both safer and superior anti-leukemic efficacy of immunotherapy in children with prognostically unfavorable population.

Acute Lymphoblastic Leukemia (ALL) in Adults vs Children: Why Such Differences in Survival
{kind=link}
{kind=link}
{kind=link}
{kind=link}