


Delighted to share ahead of #ASCO23 our contribution to the American Society of Clinical Oncology (ASCO) #EdBook where we discuss the complex considerations in the management of #cancer during #pregnancy and provide a suggested framework.
Thank you to the most wonderful mentors, Drs. Ann Partridge, Alison Loren, and Frederic Amant.
Free open-access article: https://ascopubs.org/doi/10.1200/EDBK_100037
💡 Key takeaways:
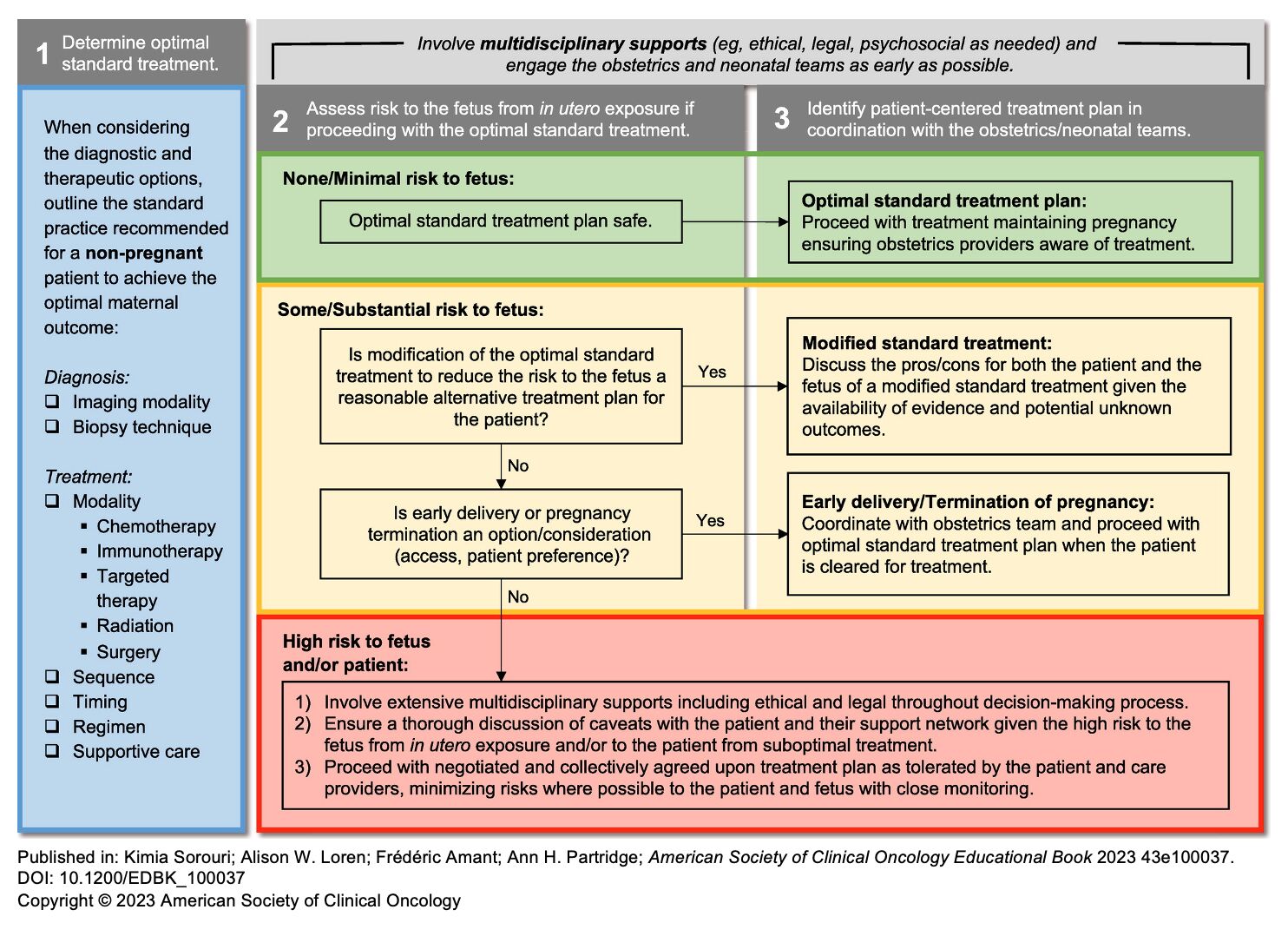
1️⃣ Cancer care during pregnancy should approximate as closely as possible to the standard treatment for a nonpregnant patient with the involvement of multidisciplinary supports, including both oncology and non-oncology medical specialists and ethical, legal, and psychosocial supports, as needed. 🤝
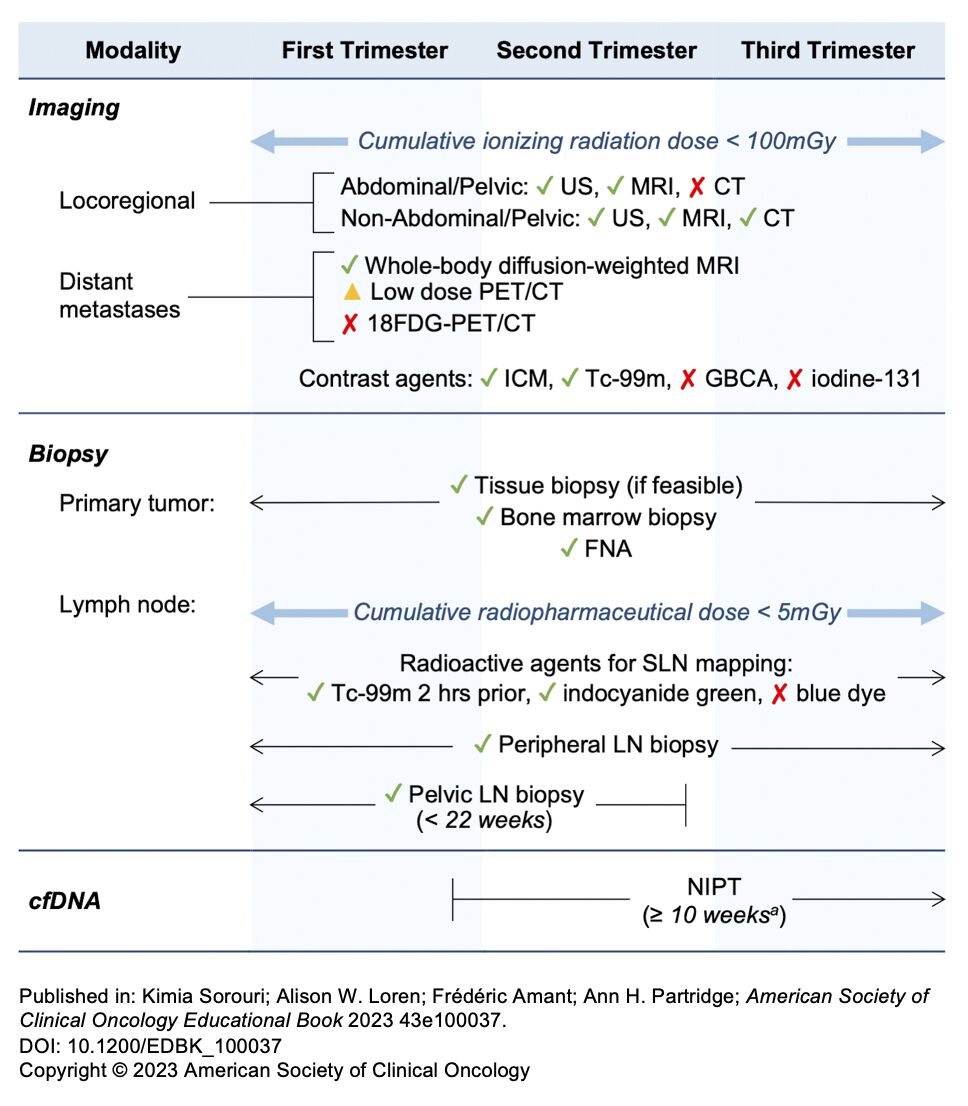
2️⃣ Ionizing radiation exposure to the fetus for diagnosis and radiotherapy, including use of radioactive agents, is to be limited to a cumulative dose of 100 mGy throughout the pregnancy. 🩻
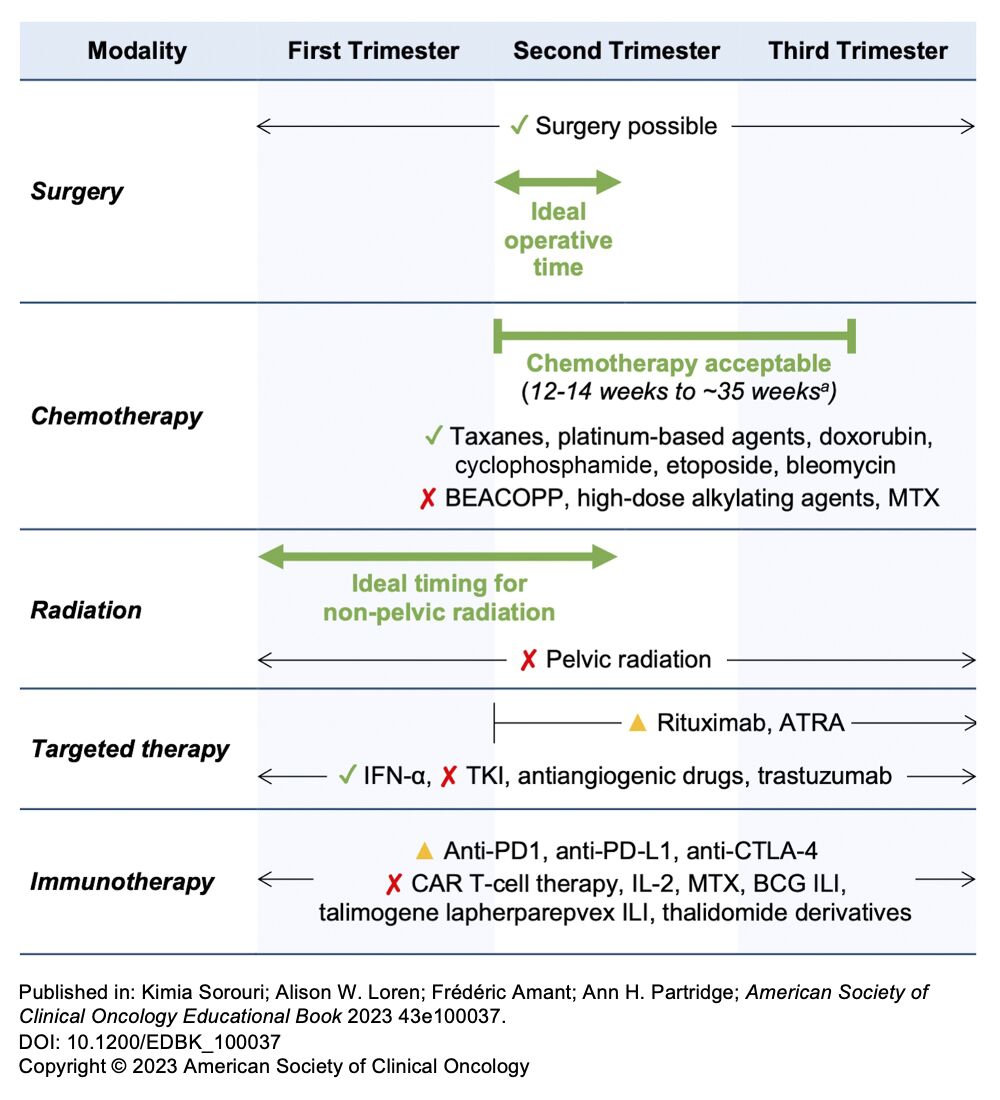
3️⃣ Risk of fetal harm with systematic therapy is greatest during the period of organogenesis; therefore, most chemotherapeutic agents can safely be administered after 12-14 weeks of gestation until 1-3 weeks before the anticipated delivery, although the use of targeted therapy and immunotherapy during pregnancy is far more restricted. 💊
4️⃣ Surgery is ideally performed during the early second trimester, although surgery can be performed throughout the entirety of pregnancy when technically feasible with additional obstetric considerations. 🪡
5️⃣ Closer prenatal monitoring is encouraged with routine biweekly fetal assessment during oncologic treatment with the goal of vaginal delivery, unless obstetrically indicated or in particular clinical scenarios, after 37 weeks of gestation when possible. 🔍
Source: Kimi Sorouri/Linkedin
{kind=link}
{kind=link}
{kind=link}
{kind=link}