


Tyler Seibert, Assistant Professor in the Division of Radiation Oncology and a member of the RMAS Center for Precision Radiation Medicine (CPRM), shared a post on X about a recent article he and his colleagues co-authored, adding:
“Important update from ProtecT Prostate Cancer trial after central pathology review
- Which early PCa need treatment? Which do not?
- For ‘bad’ early PCa, do RP or RT prevent long-term (15y) metastasis? “
Title: Active Monitoring, Surgery, and Radiotherapy for Cribriform-Positive and Cribriform-Negative Prostate Cancer. A Secondary Analysis of the PROTECT Randomized Clinical Trial
Authors: Nikita Sushentsev, Anne Y. Warren, Richard Colling, Clare Verrill, Ekaterina Pazukhina, Oleg Blyuss, Tyler M. Seibert, Tristan Barrett, Ian G. Mills, Richard J. Bryant, Jenny L. Donovan, David E. Neal, Freddie C. Hamdy
Read the Full Article on JAMA Oncology

“Central path review of available biopsy slides. N=712 participants randomized to active monitoring (AM), RT, or RP.
Outcome of interest: 15y metastasis.
Primary analysis: intention to treat.
On central path review, 42% of ProtecT participants had GG2+ cancer on biopsy (non targeted)
- ProtecT was NOT ‘only low risk’
- Population is very relevant to patients we see today

Main indicator of metastasis risk is cribriform morphology (includes all intraductal cases)
Cribriform was the only major risk factor in multivariable Cox analysis
HR 3.6 for mets
Cribriform:
- 15% overall
- 21% of GG2
- 65% of GG3

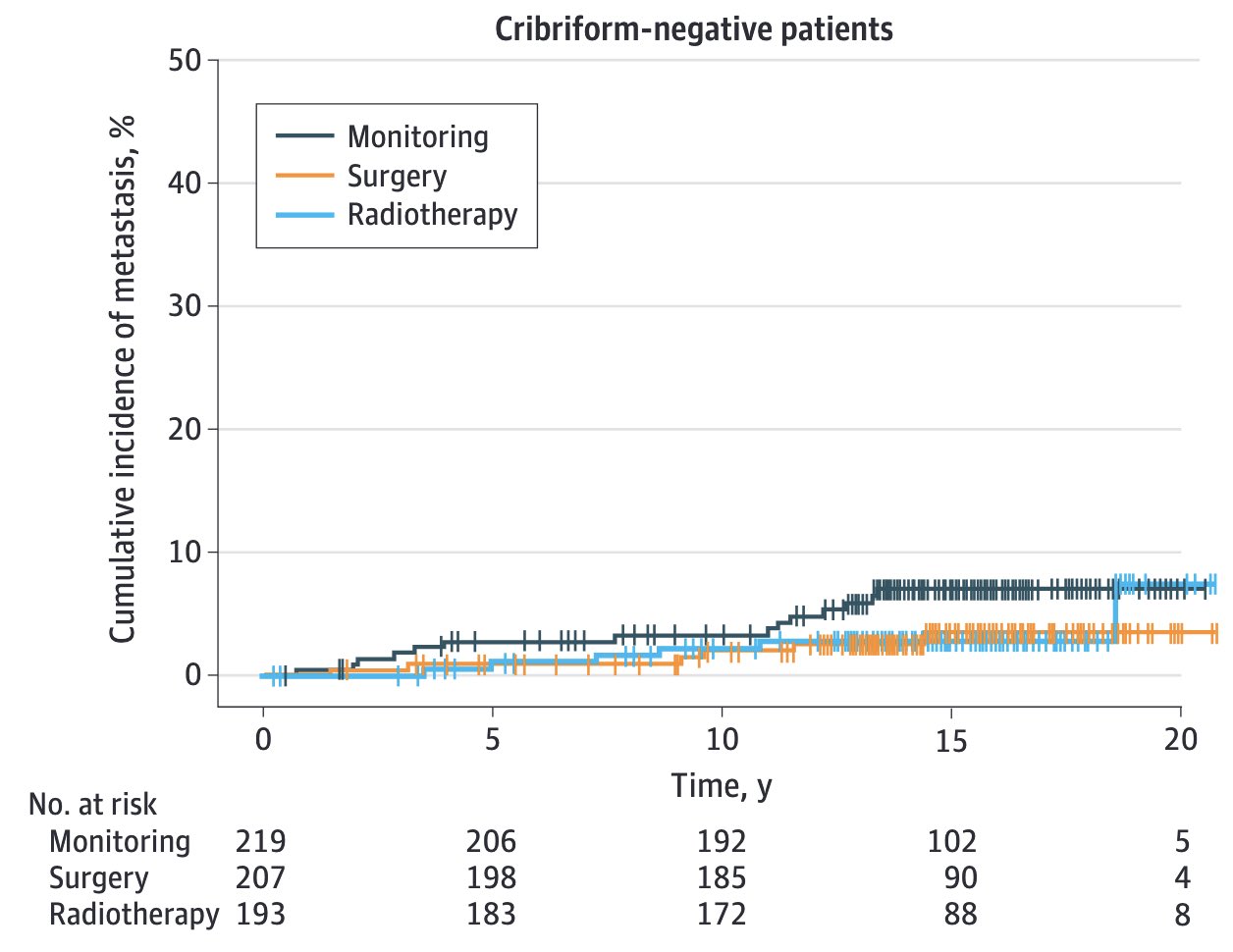
Non-cribriform Prostate Cancer does not warrant early radical therapy
Even if GG2. Look at green vs blue on 2nd figure
With MRI-guided biopsy, less bad tumors missed.
Early treatment even less likely to help today.

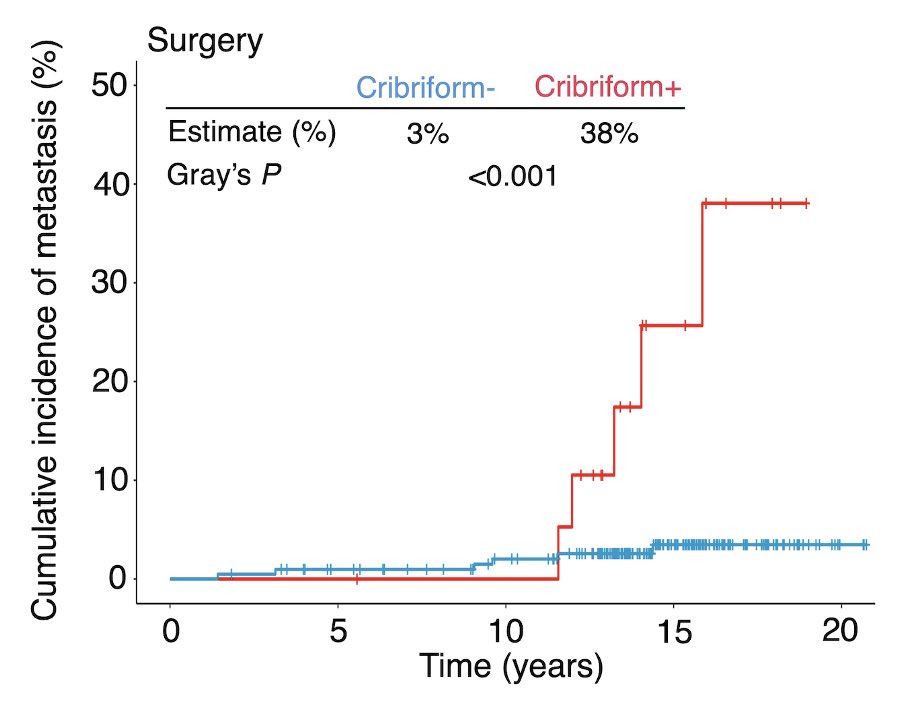
Cribriform/intraductal Prostate Cancer is not safe to monitor.
And for long-term (>10y) prevention of metastasis, multimodality treatment may be necessary.

Early treatment prevents metastatic Prostate Cancer
Small N, but at 15y:
Surgery alone controlled disease for ~10y. At 15y, metastasis rate similar to (initial) monitoring
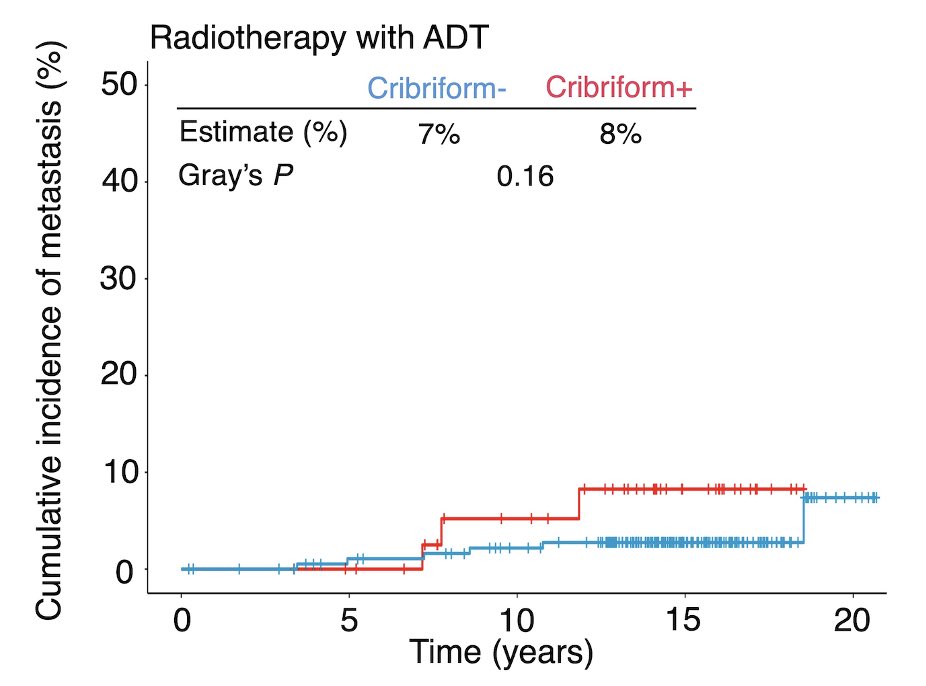
RT group had decreased mets even at 15y: they all had 3-6 mos ADT.
Per-protocol analysis to re-iterate:
No benefit to early treatment for non-cribriform GG1-2
RT + stADT highly effective at preventing metastasis even at 15y, even if crib+
RP delays mets from crib+ PCa. For 15y control, may need to optimize post-op care?

1.What about cribriform missed on biopsy? Nikita Sushentsev et al working on RP data. Stay tuned!
2.How do these results apply to modern, MRI-based AS?
3. How should we optimize multi-modal care for crib+ PCa in setting of RP?
4. Which pts benefit from RT alone?
The credit for this paper goes to Nikita Sushentsev, Freddie Hamdy and the truly fantastic ProtecT team.
Absolutely enormous honor and privilege to work w them for last 10y and to be a part of these discussions!!
Thanks to my friends for inspiration and education”
More posts featuring Tyler Seibert.
{kind=link}
{kind=link}
{kind=link}
{kind=link}