


Sara Coca Membribes, Clinical Research Fellow to Prof Powles at Barts Health NHS Trust
“First positive ph3 combining HIF-2α inhibition with immunotherapy in the adjuvant setting.
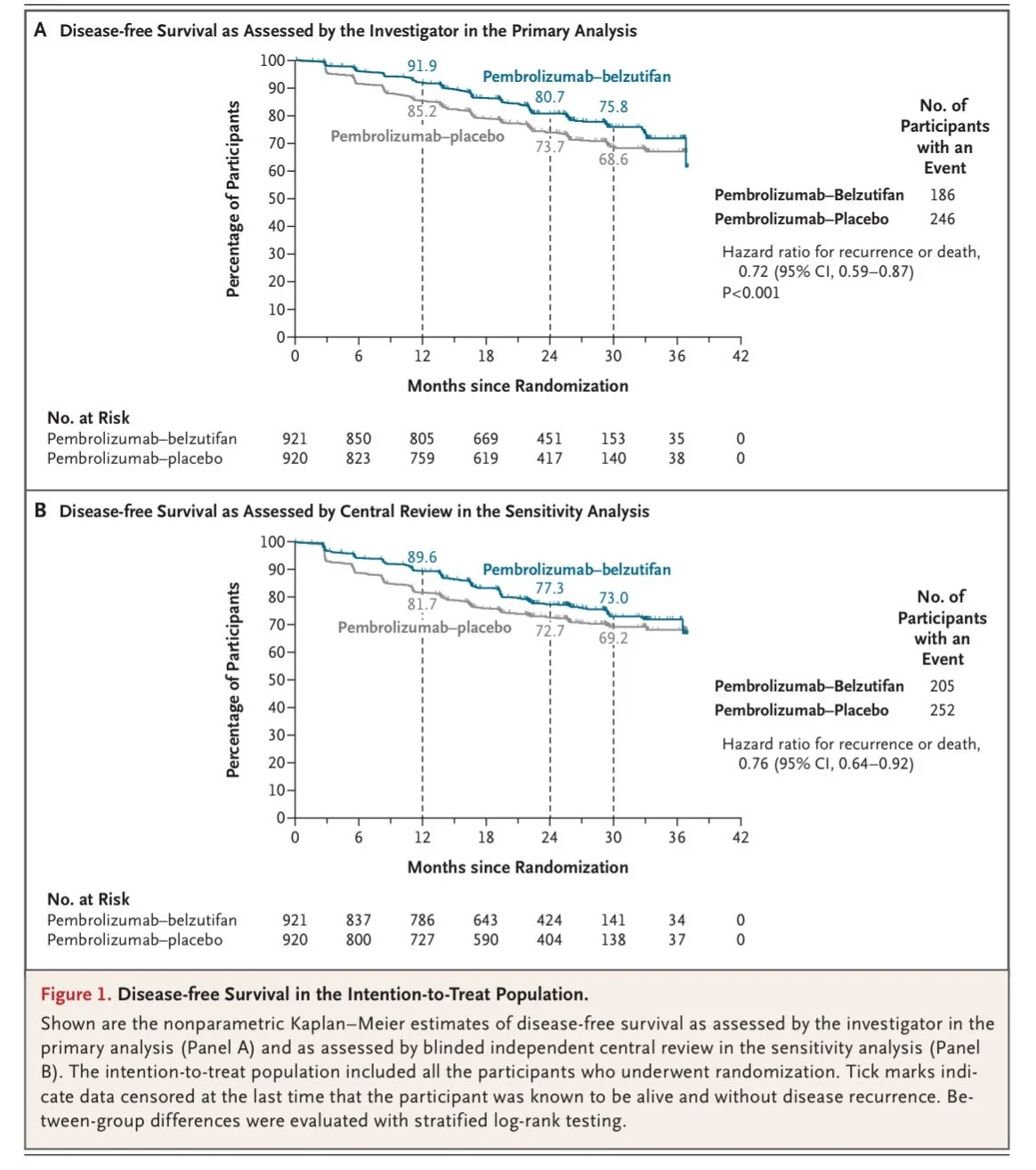
LITESPARK-022 showed high DFS with pembro + belzutifan vs pembro alone after nephrectomy for high-risk ccRCC (HR 0.72). High G3 AEs, OS immature.”

Enrique Grande, Medical Oncology Department Director at Quironsalud Madrid, Adjunct Professor at The University of Texas MD Anderson Cancer Center.
“LITESPARK-022 published in NEJM: adjuvant pembrolizumab + belzutifan vs pembrolizumab alone after nephrectomy in high-risk ccRCC (n=1,841).
24-month DFS: 80.7% vs 73.7% (HR 0.72; P<0.001). OS not yet significant at interim.
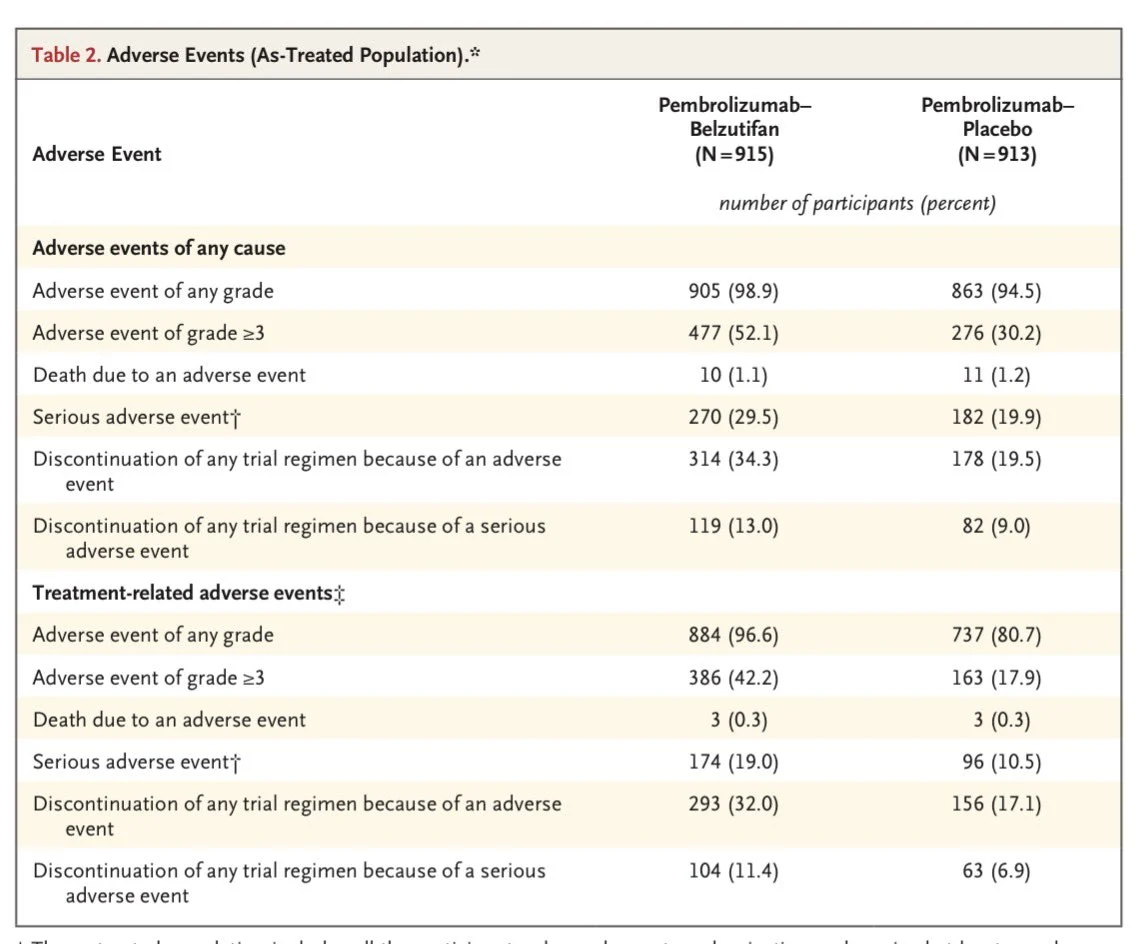
Grade ≥3 AEs: 52.1% vs 30.2% – a relevant safety signal.”

Rishabh Jain, Medical Oncologist at AIIMS.
“Adjuvant pembrolizumab alone may no longer be the ceiling in high-risk ccRCC.
LITESPARK-022 shows that adding belzutifan to adjuvant pembrolizumab after nephrectomy improves DFS in resected clear-cell RCC, but with a real toxicity cost.
Patients: intermediate-high risk, high risk, or M1 NED clear-cell RCC after surgery
Arms
Pembrolizumab + belzutifan
vs
Pembrolizumab + placebo
Efficacy
- DFS: HR 0.72 (95% CI 0.59–0.87), P<0.001
- 24-mo DFS: 80.7% vs 73.7%
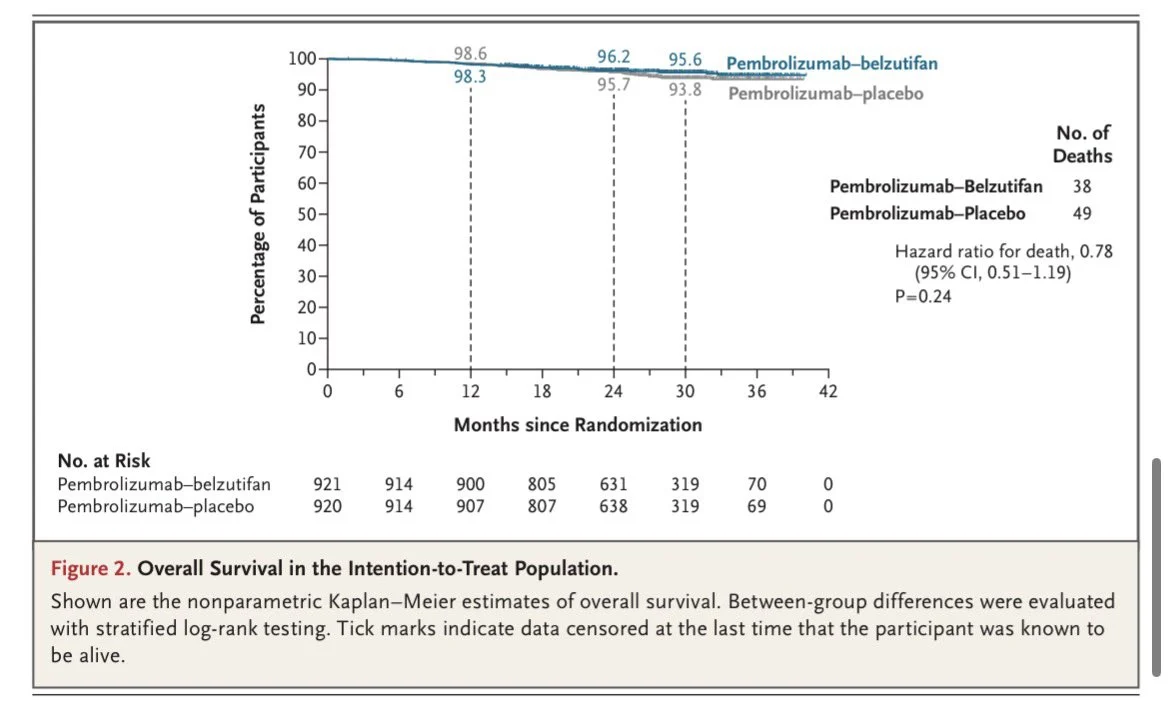
OS not mature yet
- HR 0.78 (95% CI 0.51–1.19)
- P=0.24
Toxicity
- Grade ≥3 AEs: 52.1% vs 30.2%
- Anemia: 84.0% vs 11.4%
- Hypoxia: 7.0% vs 0.1%
Bottom line:
A clear DFS-positive adjuvant RCC trial, and proof that HIF-2α inhibition can add to PD-1 blockade in earlier-stage disease.
But this is not a free intensification strategy.
The DFS gain is meaningful. The anemia burden is substantial. OS is still pending.
My read: most compelling for very high-risk / M1 NED patients, not an automatic switch for everyone on adjuvant pembrolizumab.
Would this change your adjuvant RCC practice today, or do you want OS first?”

Other articles about GU Oncology on OncoDaily.
{kind=link}
{kind=link}
{kind=link}