


Jeff Ryckman, Associate Professor of Radiation Oncology at WVU Medicine Camden Clark Medical Center, shared a post on X:
“New consensus recommendations published in Radiotherapy & Oncology provide practical guidance on focal boosting of intraprostatic tumors in prostate cancer.
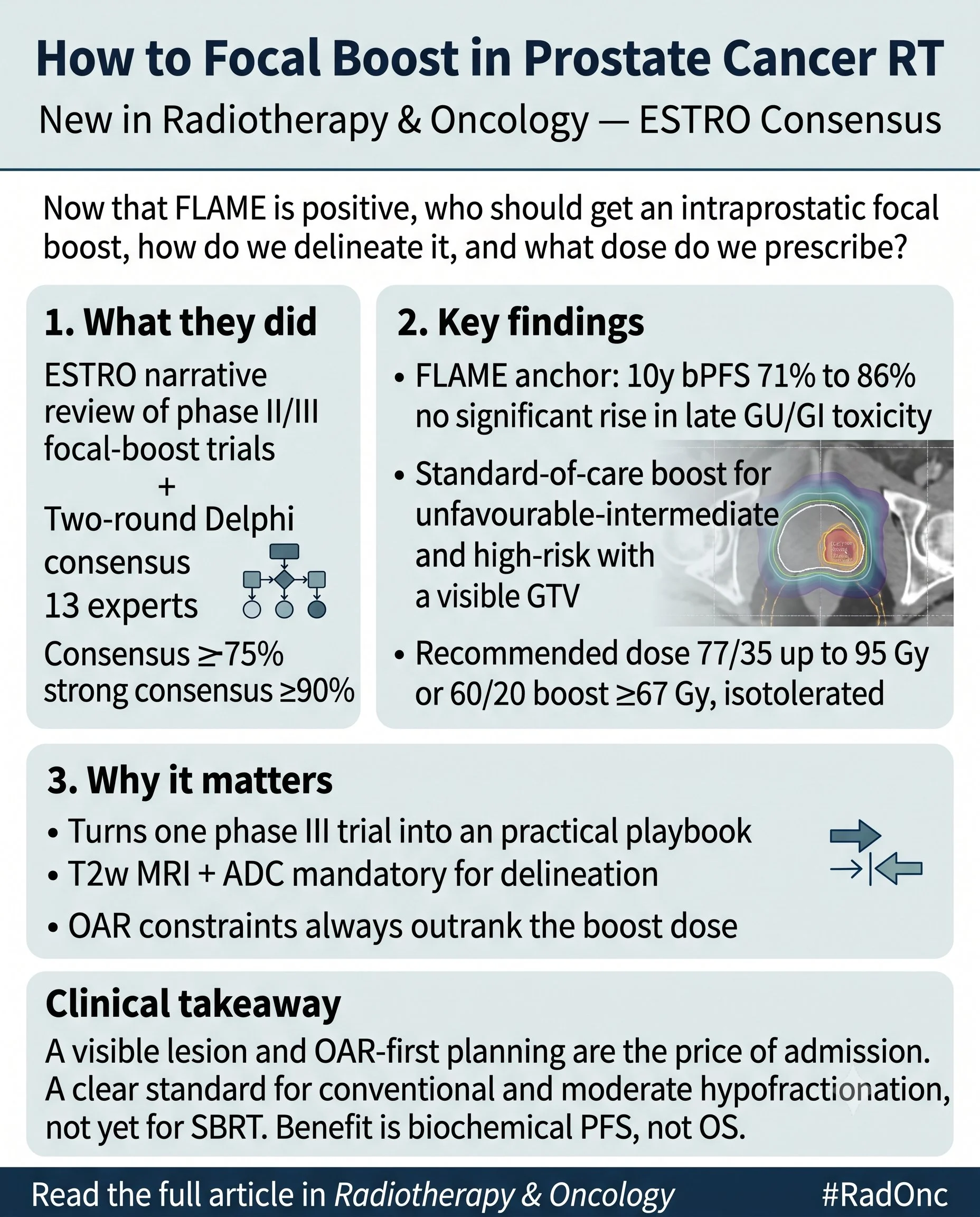
The recommendations address an important clinical question: following the positive results of the FLAME trial, which patients should receive a focal boost, how should the target be delineated, and what dose should be prescribed?
Why this matters
Focal boosting is expected to become increasingly common in the treatment of prostate cancer, making standardized guidance essential for clinical practice.
Development of the recommendations
The consensus is based on:
- A narrative review of key Phase II and Phase III focal boost trials involving at least 50 patients
- A two-round Delphi consensus process involving 13 experts, including 10 radiation oncologists, 2 medical physicists, and 1 radiation therapist (RTT)
- Consensus defined as at least 75% agreement, with strong consensus at 90% or greater
These recommendations represent expert consensus informed by existing clinical trial evidence, rather than results from a new clinical study.
Key evidence: FLAME Phase III trial (n = 571)
The FLAME study evaluated:
- 77 Gy in 35 fractions to the entire prostate
- Simultaneous integrated boost (SIB) up to 95 Gy to the gross tumor volume (GTV), while respecting normal tissue constraints
Key outcomes included:
- Five-year biochemical progression-free survival (bPFS) improved from 85% to 92%
- Ten-year bPFS improved from 71% to 86%
- No significant increase in late grade 2 or higher genitourinary (GU) or gastrointestinal (GI) toxicity
Consensus recommendations
The panel recommends:
- Focal boosting for patients with unfavorable intermediate-risk or high-risk prostate cancer who have a visible GTV
- No focal boost when no visible lesion is identified
- T2-weighted MRI and apparent diffusion coefficient (ADC) imaging as mandatory for target delineation
- PSMA PET/CT may be considered, although no consensus was reached regarding its routine use
- Dose recommendations of 77 Gy in 35 fractions with focal boost up to 95 Gy, or 60 Gy in 20 fractions with focal boost of at least 67 Gy
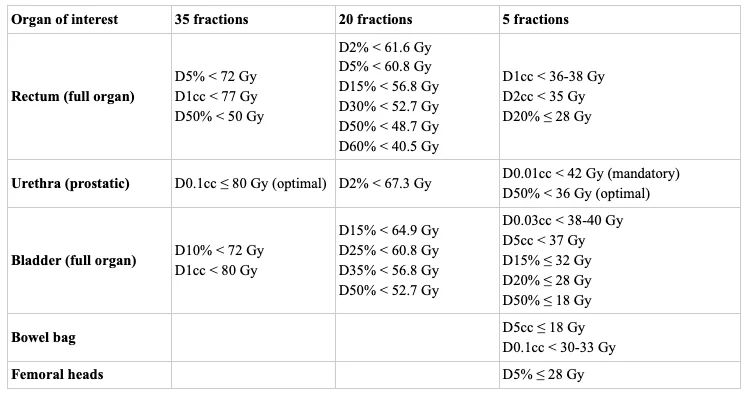
- Organ-at-risk (OAR) dose constraints should always take priority over boost dose escalation
Current limitations
The demonstrated benefit is currently improved biochemical progression-free survival.
No improvement in distant metastasis-free survival or overall survival has yet been demonstrated.
In addition, hypofractionated focal boosts and stereotactic body radiotherapy (SBRT) boost strategies are supported mainly by single-arm Phase II studies. As a result, SBRT focal boosting in fewer than five fractions remains investigational, and no consensus was reached regarding optimal SBRT boost doses.
Clinical perspective
For appropriately selected patients with visible intraprostatic tumors and unfavorable intermediate-risk or high-risk disease treated with 20- or 35-fraction radiotherapy, these recommendations provide a practical, safety-focused framework for focal boosting.
Further evidence, including toxicity data from the PIVOTALboost trial, is anticipated in 2026.”
Title: How to focal boost in prostate cancer radiotherapy: ESTRO clinical practice consensus recommendations
Authors: T. Willigenburg, C. Draulans, F. J. Pos, T. M. Seibert, I. Syndikus, A. Henry, A. Mitchell, M. Buijs, B. A. Jereczek-Fossa, S. K. B. Spohn, T. Pommer, B. R. Pieters, A. C. Tree, J. R. N. van der Voort van Zyp
Read The Full Article

Other articles about ESTRO on OncoDaily.
{kind=link}
{kind=link}