


Christine M. Lovly, Dr. Norman and Melinda Payson Professorship in Medical Oncology at City of Hope, Member Board of Directors at AACR, shared a post on LinkedIn:
“The American Society of Clinical Oncology (ASCO) Plenary is one of those rare forums where the entire global oncology community comes together around discoveries that have the potential to immediately change practice and improve patients’ lives.
Having the opportunity to serve as a discussant for the LIBRETTO-432 trial at the ASCO26 plenary was a career milestone, especially since it was shared with amazing lung cancer colleagues, Jonathan Goldman, Julie Brahmer, and Shun Lu.
LIBRETTO-432 was an international trial of adjuvant selpercatinib in RET fusion positive NSCLC. Selpercatinib significantly improved EFS in early-stage RET fusion–positive NSCLC with HR 0.172 (95% CI [0.058, 0.509]; P = 0.0003). The data speak for themselves.
In my discussion, I focused on being forward thinking. This trial will be practice changing.
What are the immediate impacts?
- A new standard of care for early-stage RET fusion-positive NSCLC.
- Proves that adjuvant studies are possible in “rare” cohorts of NSCLC.
- Early-stage molecular testing must expand.
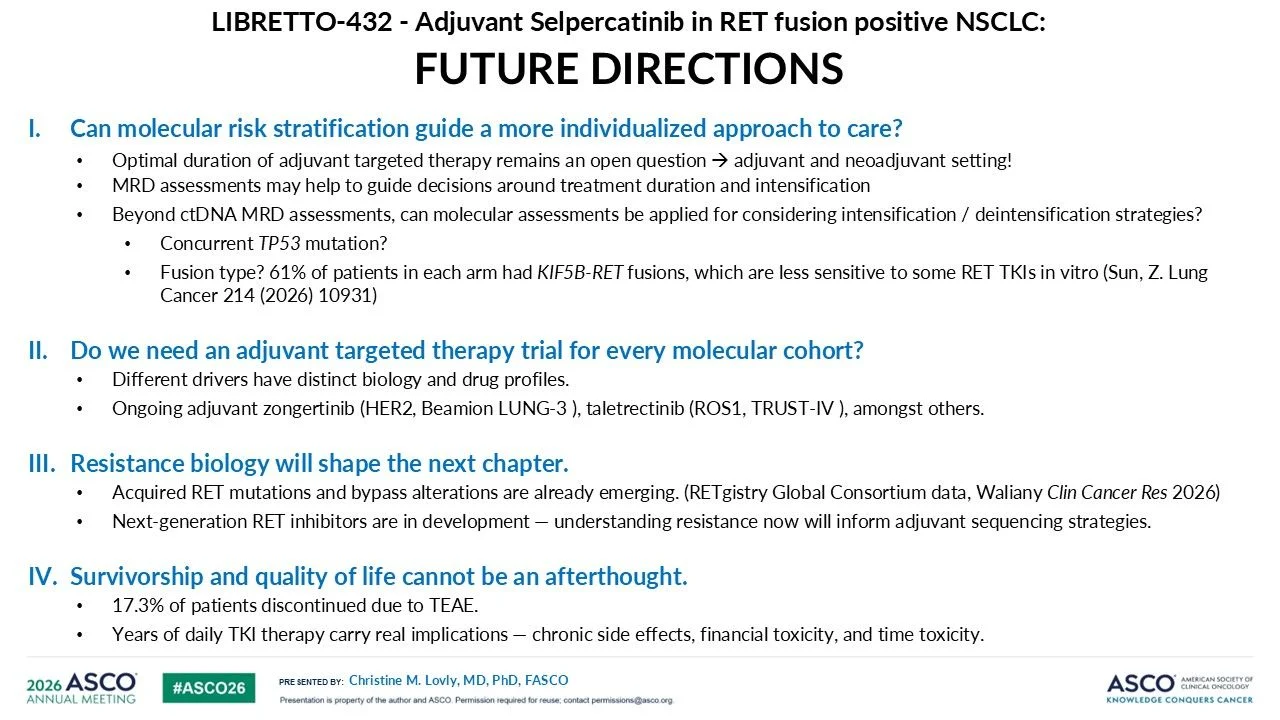
LIBRETTO-432 is an important step forward, but questions remain:
- What is the optimal duration of adjuvant targeted therapy? Eventually, MRD detection may guide individualized treatment duration – but we are not there yet.
- Does adjuvant selpercatinib improve CNS DFS? OS?
- What are the best strategies to mitigate selpercatinib tox and maximize QOL in the adjuvant setting? In LIBRETTO-432, 17.3% discontinued selpercatinib and 54.7% required dose reduction. It will be interesting to see in the future if dose reduction influenced EFS.
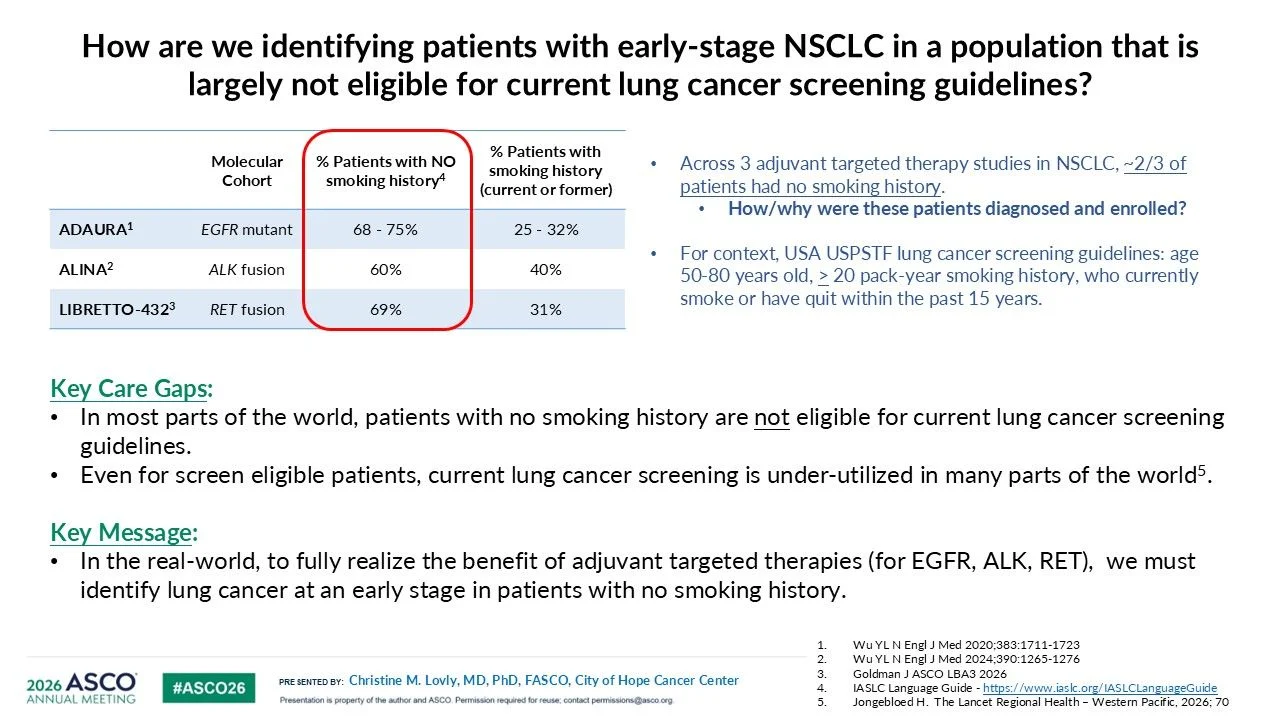
Very important question – How to identify patients with early-stage NSCLC in a population that is largely not eligible for current lung cancer screening guidelines?
- Across 3 adjuvant targeted therapy studies in NSCLC (ADAURA, ALINA, LIBRETTO-432), ~2/3 of patients had no smoking history.
How and why were these patients diagnosed and enrolled?
In the real-world, to fully realize the benefit of adjuvant targeted therapies, we must identify lung cancer at an early stage in patients with no smoking history.
Even more importantly – What do these data mean for patients?
- Access: Precision medicine fails if patients are never tested.
- Affordability: Years of adjuvant TKI therapy carry a financial burden.
- Accountability: We owe patients long-term survivorship care.
Much more to say, but running out of space! So appreciate the opportunity to present in this forum. Thank you ASCO – forever grateful!”

Other articles featuring Christine M. Lovly on OncoDaily.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}