


Anna A. Avagyan, Pediatric hematologist/oncologists at Pediatric Cancer and Blood Disorders Center of Armenia, shared a post on LinkedIn:
“Attending EHA 2026 in Stockholm, I had the opportunity yesterday to join a wonderful pediatric session: ‘Recent advances in pediatric malignancies,’ chaired by Prof. André Baruchel and Prof. Eva Fronkova.
The session gave a clear view of where pediatric hematology-oncology is moving: more precise use of MRD, earlier integration of cellular therapies, more thoughtful timing of HSCT, chemotherapy-sparing approaches, and targeted treatment based on disease biology.
Several messages stood out:
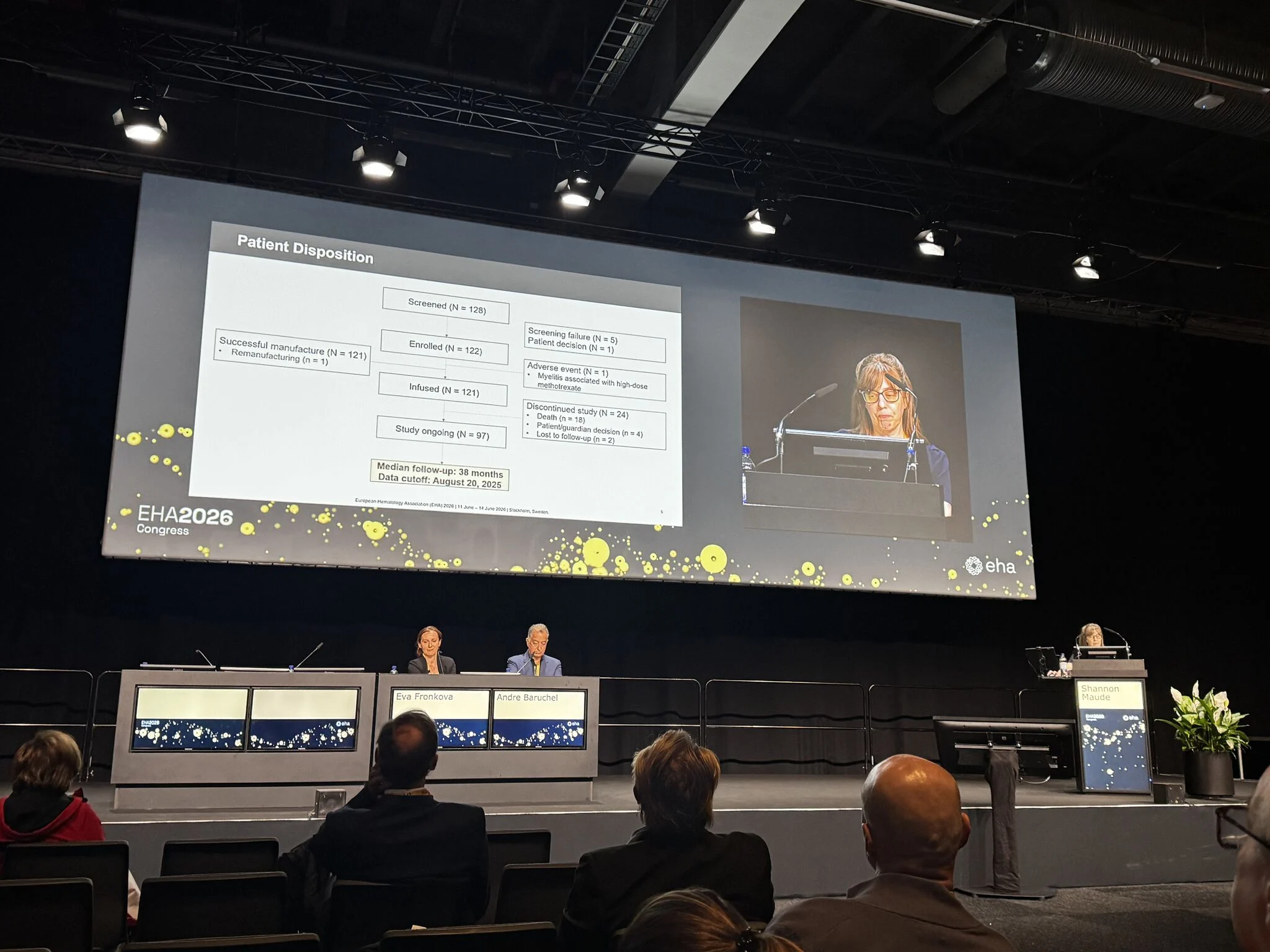
- Dr. Shannon Maude presented CASSIOPEIA/COG AALL1721, evaluating tisagenlecleucel in children and young adults with high-risk B-ALL who remained MRD-positive after frontline consolidation. The study met its primary endpoint, with an estimated 4-year overall survival of 85%, supporting CAR-T as a potentially important strategy earlier in the pathway for selected very high-risk patients.
- Dr. Lindsey Murphy addressed a practical question in pediatric AML: whether MRD-negative patients need a third chemotherapy cycle before HSCT. In this retrospective multicenter cohort, outcomes were numerically better when transplant was performed after two cycles, without a significant difference in treatment-related mortality. This is not definitive, but it raises an important question about avoiding unnecessary pre-transplant toxicity once MRD negativity is achieved.
- Prof. Franco Locatelli presented ICC-APL-02, an anthracycline-free ATRA/ATO-based approach for pediatric APL, with gemtuzumab ozogamicin added for high-risk patients. The data support the ongoing move toward chemotherapy-sparing treatment in a disease where cure rates are high and long-term toxicity matters.
- Dr. Rui Zhang presented luvometinib in recurrent/refractory pediatric Langerhans cell histiocytosis. The response and disease control rates were high, with encouraging 12-month PFS during treatment and an acceptable safety profile. As a single-arm study, longer follow-up will be important, especially after treatment discontinuation.
- Dr. Vincenzo Giambra presented translational work showing how EZH2 loss and HOXA9-mediated reprogramming may contribute to high-risk ETP-ALL biology and help identify poorer-prognosis T-ALL subgroups.
My main conclusion: pediatric malignancy care is becoming increasingly response-adapted, biology-driven, and toxicity-conscious. The key challenge now is not only developing new therapies, but integrating them carefully into real-world treatment pathways where efficacy, safety, access, and long-term outcomes are all considered.
For clinical practice, the key question is increasingly not only ‘what treatment can we add?’ but also ‘which treatment is truly necessary for this child, at this moment, based on response and biology?'”

More posts featuring Anna A. Avagyan.
{kind=link}