

1 Rechallenge in Advanced NSCLC: A Small Signal, but Not a New Standard 1")
Immune checkpoint inhibitors changed the treatment landscape for advanced non-small cell lung cancer. Yet for most patients, resistance eventually develops.
After progression on a PD-1 or PD-L1 inhibitor, clinicians face a difficult question: can immunotherapy work again?
A new systematic review and meta-analysis examined PD-(L)1 inhibitor rechallenge strategies in patients with advanced NSCLC previously treated with immunotherapy. The analysis brings together the largest body of evidence to date, including randomized trials and more than 100 non-randomized studies.
The overall message is cautious.
Across randomized studies, PD-(L)1 rechallenge produced statistically significant but clinically modest improvements in overall and progression-free survival compared with standard chemotherapy. There was no meaningful improvement in objective response rate.
The more interesting signal emerged in patients with features of acquired resistance to prior immunotherapy. In this subgroup, rechallenge appeared more promising. However, the evidence remains exploratory and is not sufficient to support broad use in routine practice.
1 Rechallenge in Advanced NSCLC: A Small Signal, but Not a New Standard 2")
What Is PD-(L)1 Rechallenge?
PD-(L)1 rechallenge refers to reintroducing or continuing PD-1 or PD-L1 blockade after a patient has progressed on a prior immunotherapy-containing regimen.
This strategy has been tested in several ways. Some trials combined a PD-(L)1 inhibitor with chemotherapy. Others added antiangiogenic agents, tyrosine kinase inhibitors, novel immune modulators, or dual-checkpoint approaches.
The biological rationale is understandable. Resistance to immunotherapy is not always absolute. Some tumors may retain partial immune sensitivity, while a new treatment partner could alter the tumor microenvironment and restore activity.
However, the clinical evidence has been inconsistent.
A major challenge is that patients who progress early on immunotherapy may be biologically very different from those who initially respond and later develop resistance.
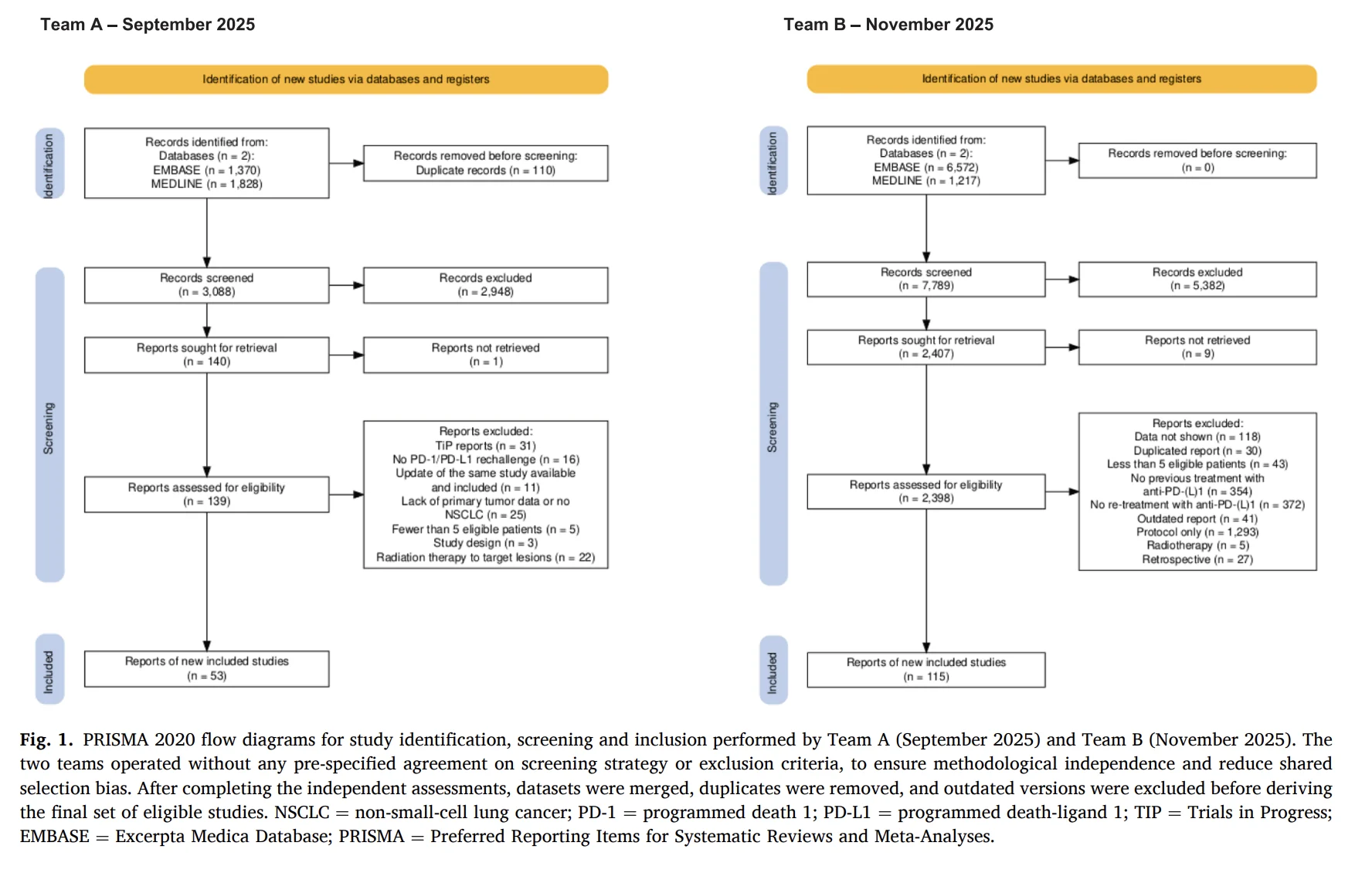
What Did the Meta-Analysis Include?
The review identified 116 interventional studies in total.
This included:
- 10 randomized controlled trials
- 3,081 patients in the randomized evidence base
- 106 non-randomized single-arm trials
The randomized studies compared PD-(L)1-based rechallenge combinations with standard treatment approaches, most commonly docetaxel-based chemotherapy, docetaxel plus ramucirumab, or investigator’s choice chemotherapy.
The authors focused on overall survival as the primary endpoint. Progression-free survival, objective response rate, and safety were also assessed.
1 Rechallenge in Advanced NSCLC: A Small Signal, but Not a New Standard 3")
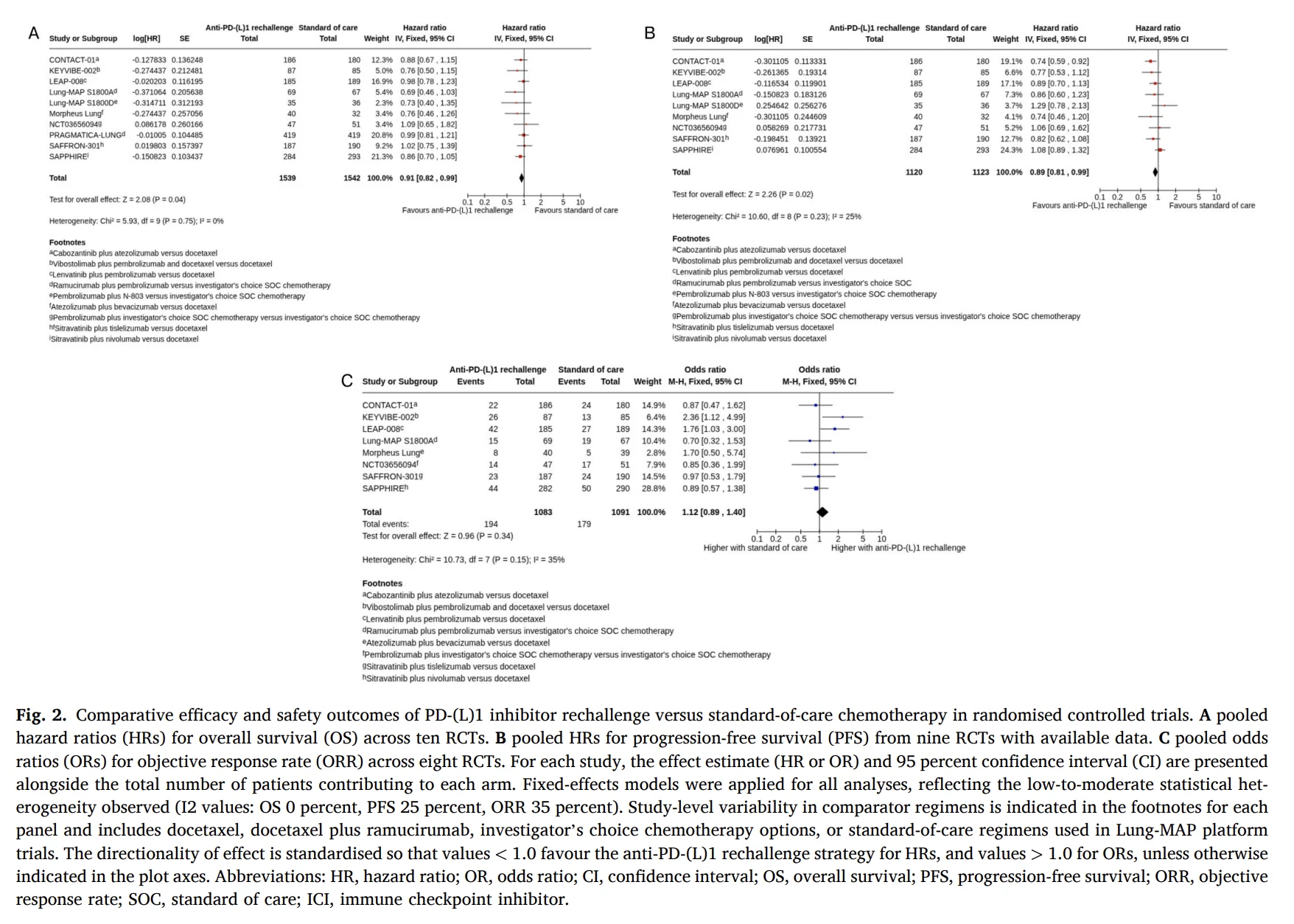
Did PD-(L)1 Rechallenge Improve Survival?
Across the 10 randomized trials, PD-(L)1 rechallenge strategies were associated with a modest improvement in overall survival.
The pooled overall survival hazard ratio was 0.91. This reflected a small reduction in the risk of death compared with control treatment.
Progression-free survival also showed a statistically significant but modest advantage, with a pooled hazard ratio of 0.89.
At first glance, these results may appear encouraging. However, the authors emphasize that the magnitude of benefit was limited and did not represent a clinically meaningful survival advantage for the overall population.
Most individual trials did not demonstrate a clear survival benefit on their own. Confidence intervals frequently crossed unity, and results varied across different treatment backbones.
In other words, the meta-analysis detected a small pooled effect, but not a consistent result strong enough to redefine second-line treatment after chemoimmunotherapy.
Objective Responses Did Not Improve
The analysis found no meaningful improvement in objective response rate with PD-(L)1 rechallenge.
Across eight randomized trials, the pooled odds ratio for objective response rate was 1.12, with a confidence interval crossing one.
This suggests that rechallenge did not consistently increase the likelihood of measurable tumor shrinkage compared with standard treatments.
That matters clinically. In the post-immunotherapy setting, patients often need rapid disease control. A regimen that does not reliably improve response rates may have limited value for individuals with symptomatic disease or high disease burden.
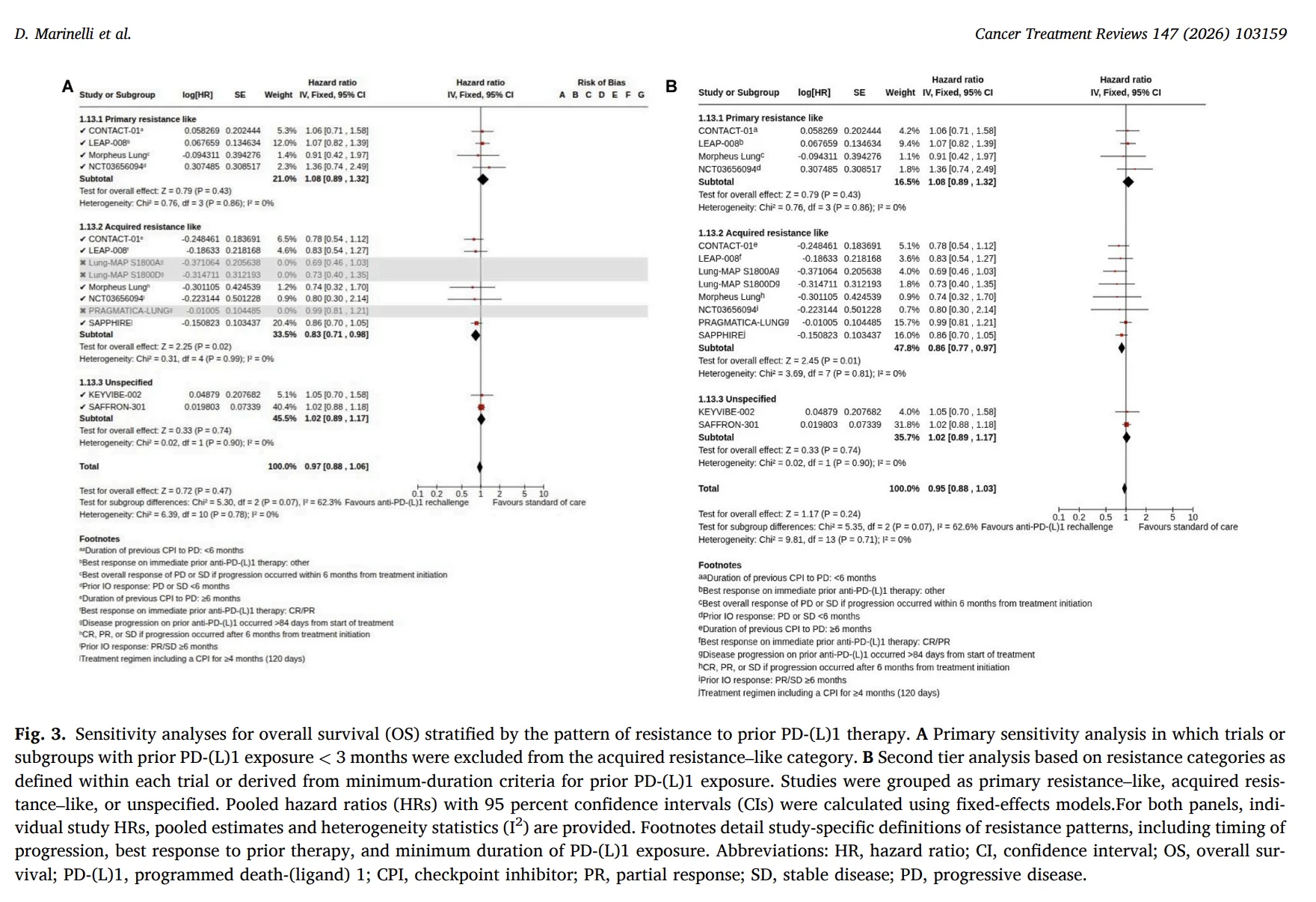
Why Does Resistance Pattern Matter?
The most important finding was linked to the pattern of resistance to prior immunotherapy.
The authors separated patients into groups with features resembling primary resistance or acquired resistance.
Primary resistance generally refers to disease progression with little or no meaningful benefit from initial immunotherapy. Acquired resistance occurs after a period of response or durable disease control, followed by eventual progression.
In the primary resistance-like subgroup, PD-(L)1 rechallenge did not show a survival benefit.
By contrast, patients with features of acquired resistance had a more favorable overall survival signal. In the analysis using trial-reported resistance categories or minimum prior exposure criteria, the pooled overall survival hazard ratio was 0.86.
This suggests that patients who previously derived clinical benefit from immunotherapy may be more likely to benefit from a rechallenge strategy than those whose disease was immunotherapy-refractory from the beginning.
Still, this result must be interpreted carefully.
Definitions of primary and acquired resistance differed across trials. Some studies used duration of prior immunotherapy exposure. Others used best response or time to progression. The interaction test between subgroups was not statistically significant.
Therefore, acquired resistance is not yet a validated biomarker for selecting PD-(L)1 rechallenge in clinical practice.
1 Rechallenge in Advanced NSCLC: A Small Signal, but Not a New Standard 4")
Why Might Acquired Resistance Behave Differently?
Primary resistance may reflect a tumor microenvironment that was never effectively recognized by the immune system.
These tumors may have limited T-cell infiltration, defective antigen presentation, impaired interferon signaling, or other features associated with an immune-cold phenotype.
Acquired resistance is different. It develops after a period of immune control.
In these tumors, the cancer may adapt through immune escape mechanisms, changes in antigen presentation, T-cell exhaustion, alternative checkpoint activation, or immunosuppressive signaling pathways.
This creates a potential opportunity. If some immune sensitivity remains, a new combination strategy may help restore activity.
The present analysis does not prove this mechanism. But it supports the need for future trials that prospectively distinguish between primary and acquired resistance.
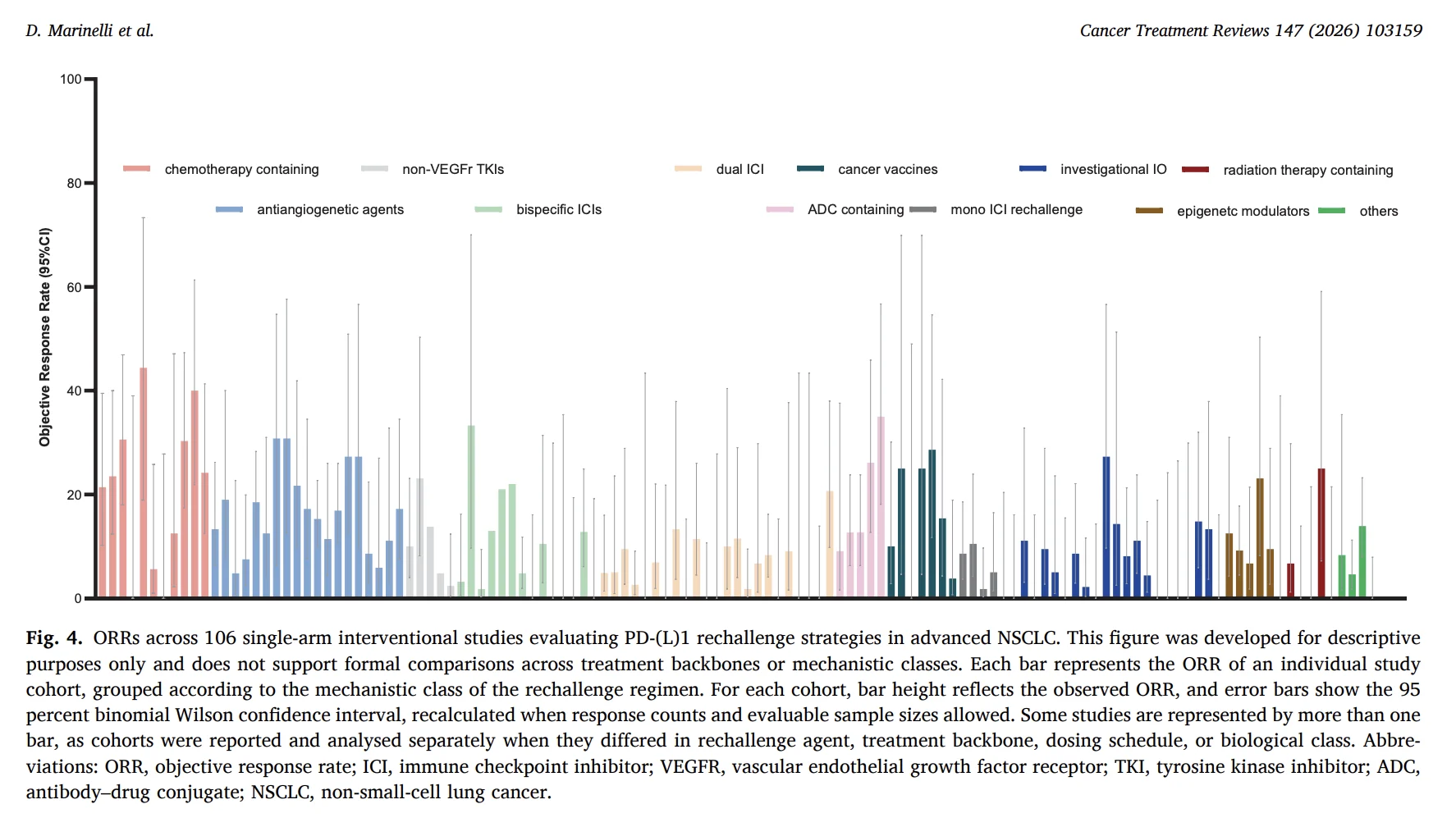
Were Any Rechallenge Strategies More Promising?
The 106 single-arm studies showed highly variable response rates.
Some chemotherapy-containing and VEGF-targeting regimens appeared to have somewhat higher response signals. However, these observations were inconsistent and must not be interpreted as comparative evidence.
The studies differed widely in patient populations, treatment partners, prior immunotherapy exposure, resistance definitions, sample size, and outcome reporting.
No robust activity signal emerged for dual immune checkpoint combinations, bispecific antibodies, investigational immunotherapies, ADC-containing regimens, cancer vaccines, or epigenetic therapies.
The review also noted that toxicity varied substantially according to the accompanying treatment backbone.
Multitarget tyrosine kinase inhibitor combinations were generally associated with a greater burden of grade 3–5 treatment-related adverse events than chemotherapy-free or antibody-based regimens.
What Does This Mean for Current Practice?
The findings do not support routine PD-(L)1 rechallenge for all patients with advanced NSCLC who progress after chemoimmunotherapy.
The authors conclude that docetaxel, with or without ramucirumab, remains the standard second-line approach for patients without actionable oncogenic drivers.
PD-(L)1 rechallenge should currently be pursued within clinical trials, ideally in biologically or clinically enriched populations.
This is especially important because the randomized evidence evaluated combination strategies. It is impossible to fully separate the contribution of renewed PD-(L)1 blockade from the effect of chemotherapy, antiangiogenic treatment, tyrosine kinase inhibition, or another added drug.
1 Rechallenge in Advanced NSCLC: A Small Signal, but Not a New Standard 5")
What Should Future Trials Do Differently?
The key need is better patient selection.
Future studies should use harmonized definitions of resistance that incorporate duration of prior benefit, depth of response, timing of progression, and treatment-free interval.
Dynamic biomarkers may also be needed. Static PD-L1 expression at rechallenge did not identify patients likely to benefit in this analysis.
More informative approaches may include longitudinal tumor profiling, circulating tumor DNA, antigen-presentation pathways, interferon-gamma signaling, immune-cell states, and markers of T-cell exhaustion.
The question may not be whether PD-(L)1 rechallenge works in NSCLC overall.
The more relevant question is: which patients still have enough residual immune sensitivity for rechallenge to matter?
The Bottom Line
PD-(L)1-based rechallenge after prior immunotherapy in advanced NSCLC produced only marginal survival improvements overall and did not improve objective response rates.
The strategy showed no clear benefit for patients with primary resistance.
A more favorable, but still exploratory, survival signal was observed among patients with features of acquired resistance to prior immunotherapy.
For now, PD-(L)1 rechallenge remains a research strategy rather than a standard approach. Its future may depend on resistance-aware trial designs and biomarkers that distinguish truly refractory disease from tumors that retain partial immune sensitivity.
{kind=link}
{kind=link}
{kind=link}
{kind=link}