


Dual immune checkpoint blockade with nivolumab plus ipilimumab can provide durable, long-term benefit for some patients with metastatic non-small cell lung cancer. However, immunotherapy does not benefit every patient at the same pace.
A new exploratory analysis of the phase III CheckMate 227 and CheckMate 9LA trials examined an important clinical concern: early detriment after starting first-line nivolumab plus ipilimumab–based treatment.
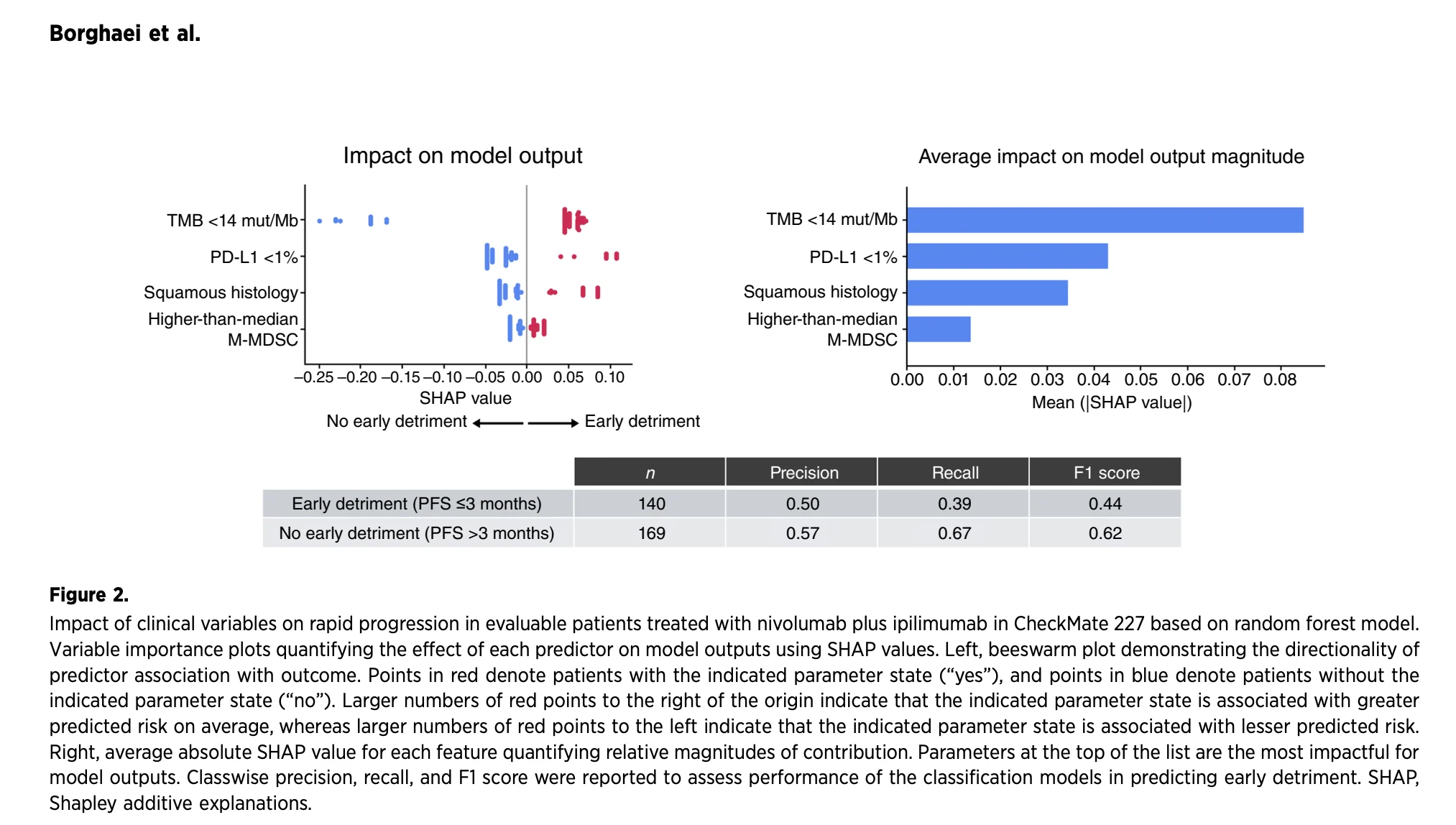
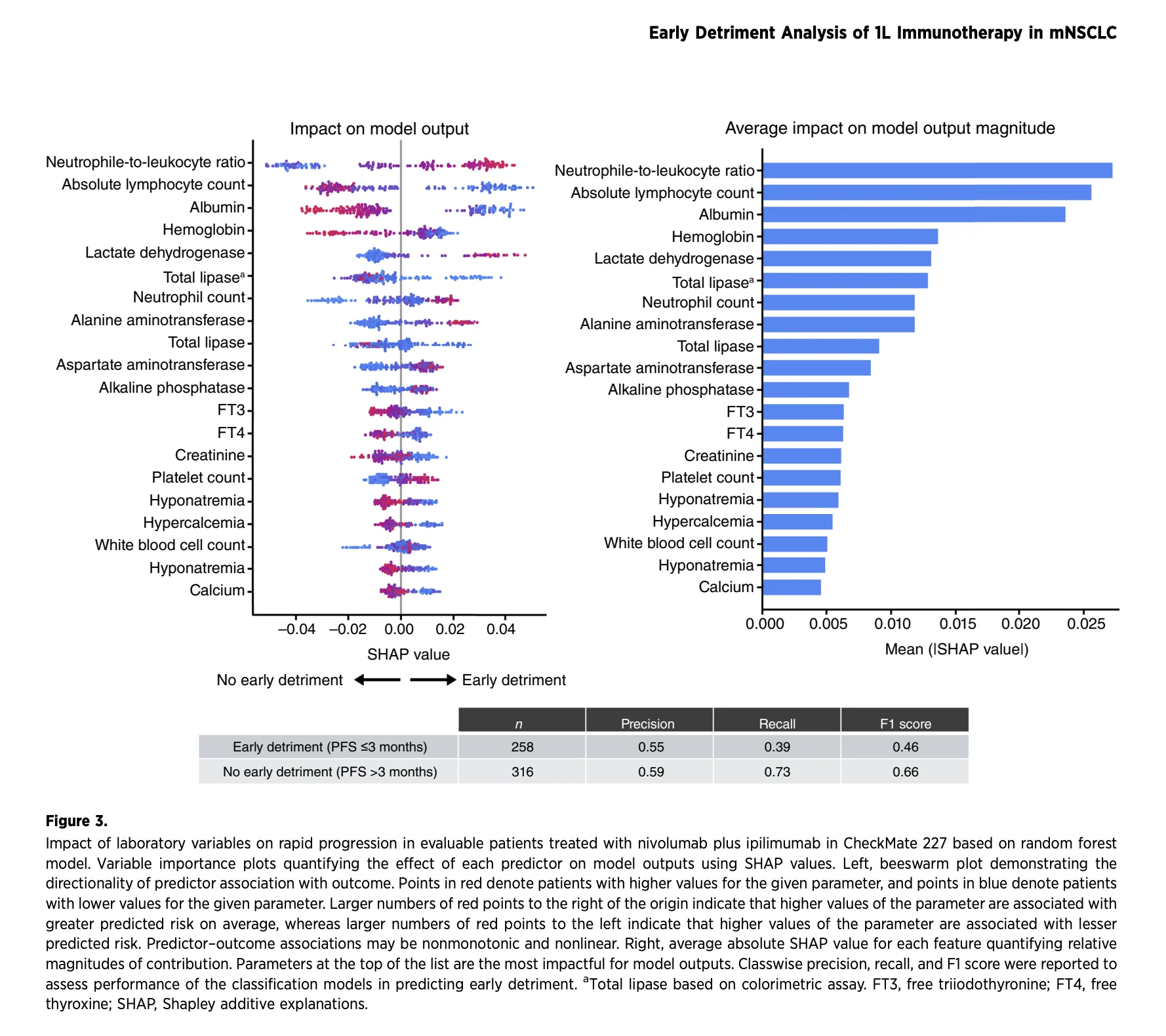
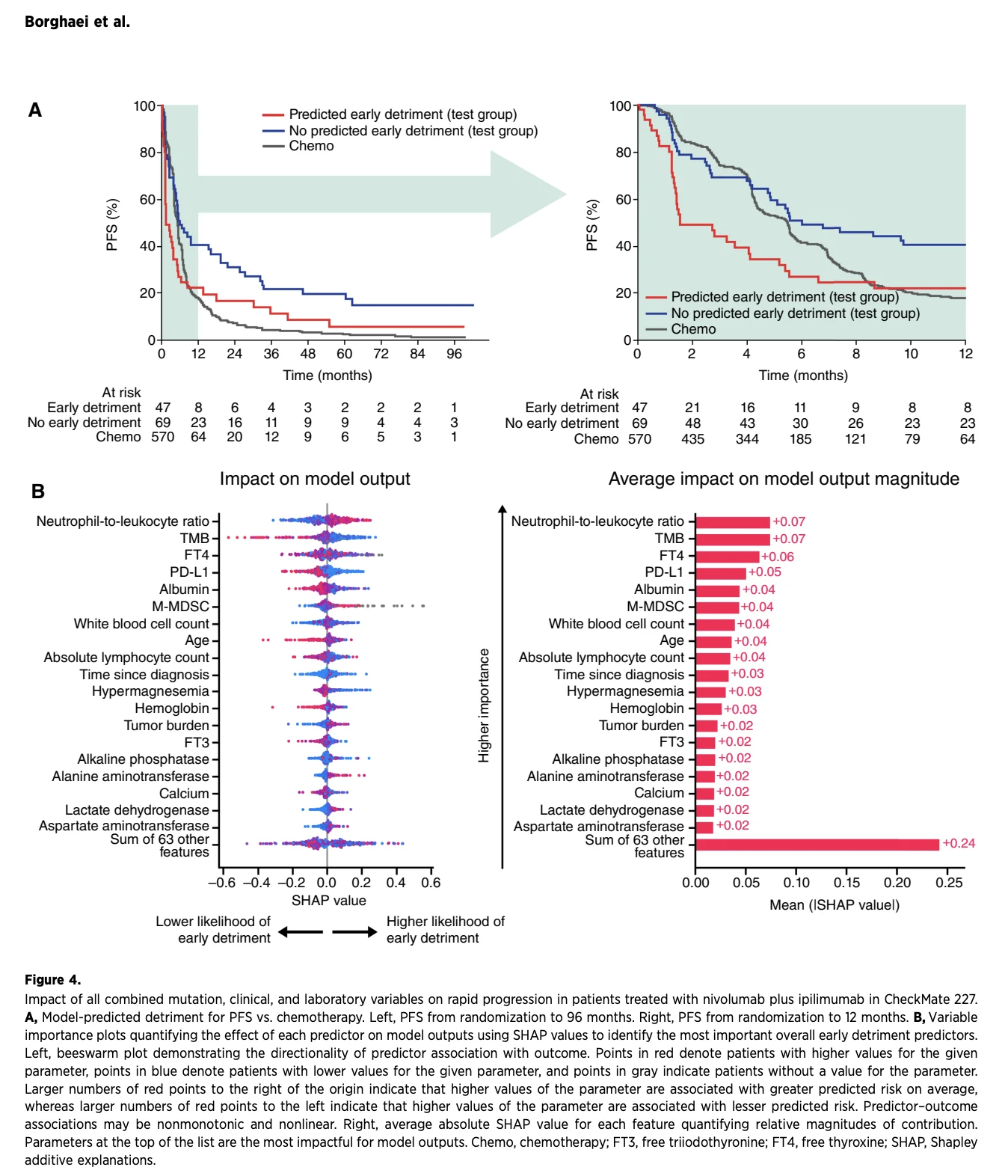
The analysis found that rapid progression was more common with nivolumab plus ipilimumab alone than with chemotherapy in CheckMate 227. Several baseline factors were associated with this early risk, including high neutrophil-to-leukocyte ratio, low tumor mutational burden, low PD-L1 expression, low albumin, and higher baseline monocytic myeloid-derived suppressor cell levels.
Importantly, the same pattern was not observed when nivolumab plus ipilimumab was combined with two cycles of chemotherapy in CheckMate 9LA.

What Did the Researchers Define as Early Detriment?
The study defined rapid progression as disease progression or death within three months of randomization. Early death was defined as death from any cause within the same three-month period.
The analysis focused on patients with metastatic NSCLC without sensitizing EGFR mutations or ALK rearrangements who were treated in the CheckMate 227 or CheckMate 9LA trials.
CheckMate 227 compared first-line nivolumab plus ipilimumab with chemotherapy. CheckMate 9LA compared nivolumab plus ipilimumab combined with two cycles of platinum-doublet chemotherapy with chemotherapy alone.
The aim was not only to identify patients who may experience early progression with dual immunotherapy, but also to understand whether adding chemotherapy could reduce this early-risk period.
Rapid Progression Was More Common With Nivolumab Plus Ipilimumab Alone
In CheckMate 227, 1,166 patients were randomized to nivolumab plus ipilimumab or chemotherapy.
Rapid progression occurred in 40% of patients receiving nivolumab plus ipilimumab, compared with 26% of patients receiving chemotherapy.
Early death occurred in 13% of patients treated with nivolumab plus ipilimumab and 10% of those treated with chemotherapy.
The progression-free survival curves initially favored chemotherapy, with nivolumab plus ipilimumab beginning to show improvement after approximately three months. This pattern reflects a well-recognized challenge with immunotherapy-only strategies: a subgroup of patients may experience disease progression before a durable immune response has time to develop.
Still, the long-term benefit of nivolumab plus ipilimumab remained evident. Across longer follow-up, the regimen continued to provide durable disease control and survival benefit in selected patients.

Which Factors Were Linked With Rapid Progression?
The investigators used multivariable models that included mutation-related, clinical, and laboratory variables.
Several baseline characteristics were associated with a higher likelihood of rapid progression during nivolumab plus ipilimumab treatment:
- High neutrophil-to-leukocyte ratio
- Tumor mutational burden below 14 mutations per megabase
- Tumor PD-L1 expression below 1%
- Low albumin level
- Higher-than-median monocytic myeloid-derived suppressor cell level
- Among these variables, neutrophil-to-leukocyte ratio, tumor mutational burden, PD-L1 expression, albumin, and monocytic myeloid-derived suppressor cell level were among the most important factors in the combined model.
These findings suggest that early failure of dual immunotherapy may be related to several overlapping factors: limited tumor immunogenicity, systemic inflammation, poor nutritional or inflammatory status, and an immunosuppressive circulating immune environment.
Tumor Mutational Burden Was a Key Signal
Tumor mutational burden was one of the strongest clinical variables associated with rapid progression.
Among patients with TMB below 14 mutations per megabase in CheckMate 227, rapid progression occurred in 47% of patients receiving nivolumab plus ipilimumab, compared with 28% of those receiving chemotherapy.
By contrast, in patients with TMB of at least 14 mutations per megabase, rapid progression occurred in 21% of patients treated with nivolumab plus ipilimumab and 20% of those receiving chemotherapy.
Across the full follow-up period, progression-free survival favored nivolumab plus ipilimumab in the high-TMB group. In the low-TMB group, progression-free survival was similar between nivolumab plus ipilimumab and chemotherapy.
These findings do not establish TMB as a standalone treatment-selection biomarker. However, they reinforce the idea that patients with lower TMB may be less likely to experience early benefit from immunotherapy-only treatment.
PD-L1 Alone Was Not Enough
Low PD-L1 expression was identified as a contributor to rapid progression in the multivariable analysis. However, PD-L1 alone did not fully explain early detriment.
In CheckMate 227, rapid progression rates with nivolumab plus ipilimumab were similar among patients with PD-L1 expression below 1% and those with PD-L1 expression of at least 1%.
This is an important finding because it shows why treatment decisions should not rely on one biomarker in isolation. PD-L1 expression, TMB, inflammatory markers, albumin, immune-suppressive myeloid cells, disease burden, and clinical condition may all interact.
The authors suggest that combining variables in a multimodal model may be more informative than considering any single marker independently.

What Did Long-Term Survivors Look Like?
The study also compared patients with rapid progression and patients who survived for at least five years after nivolumab plus ipilimumab treatment.
Long-term survivors had higher average PD-L1 expression and higher baseline TMB. They also had lower neutrophil-to-leukocyte ratios and lower baseline monocytic myeloid-derived suppressor cell levels.
This inverse relationship supports the biological relevance of the identified risk factors. Patients with more favorable immune and inflammatory profiles appeared more likely to achieve durable benefit from dual immunotherapy.
Did Chemotherapy Change the Early-Risk Pattern?
The most clinically relevant finding came from CheckMate 9LA.
In this trial, patients received nivolumab plus ipilimumab together with two cycles of chemotherapy. Rapid progression occurred in 27% of patients receiving the combination, compared with 28% of patients receiving chemotherapy alone.
Early death occurred in 10% of patients receiving nivolumab plus ipilimumab plus chemotherapy and 11% of those receiving chemotherapy alone.
Unlike CheckMate 227, the addition of chemotherapy did not show an increased rate of early detriment compared with chemotherapy alone across the evaluated biomarker-defined subgroups.
This may suggest that chemotherapy helps provide early disease control while nivolumab plus ipilimumab works to generate a longer-term immune response. Chemotherapy may reduce tumor burden rapidly, alter the tumor microenvironment, and potentially support immune-mediated antitumor activity.
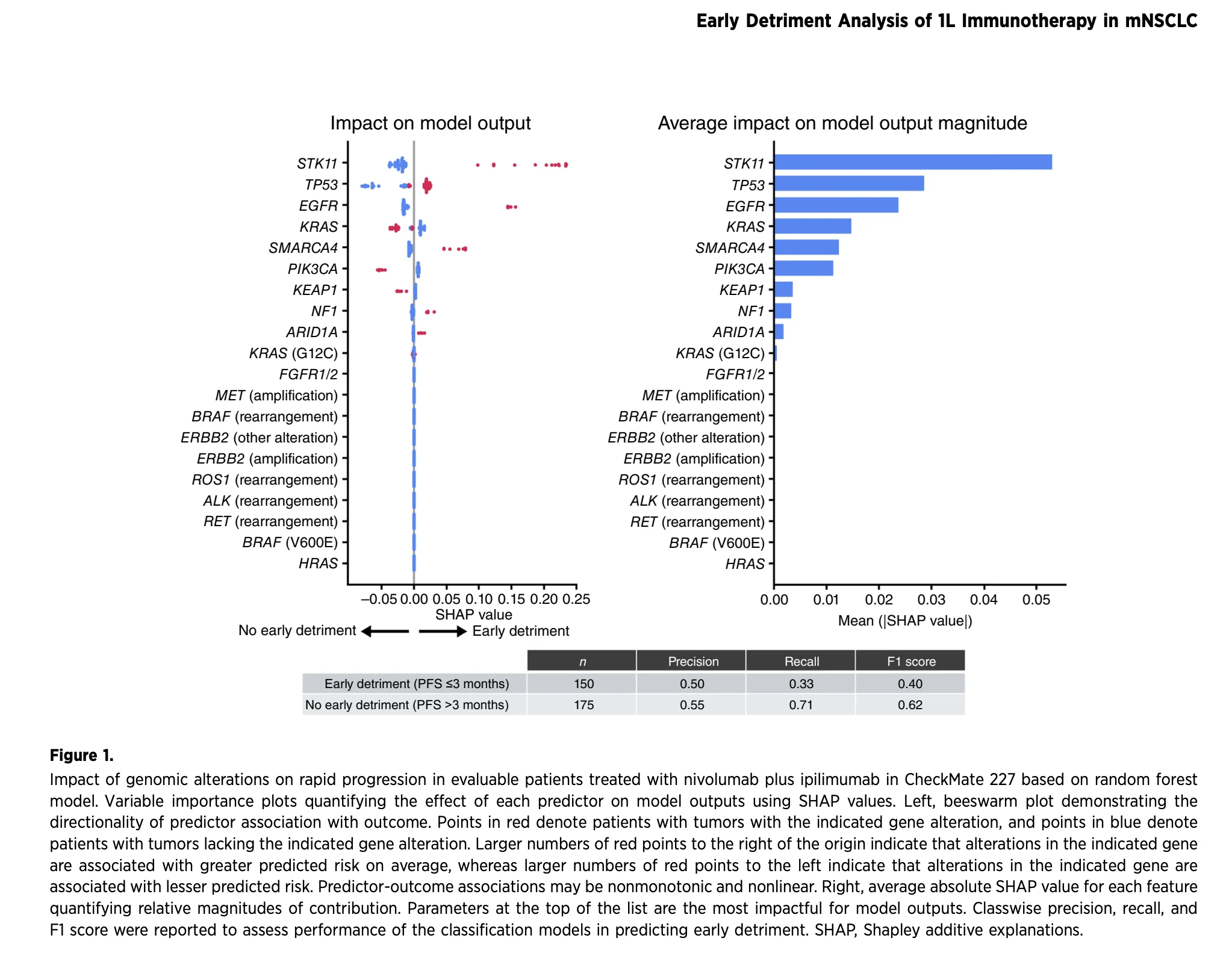
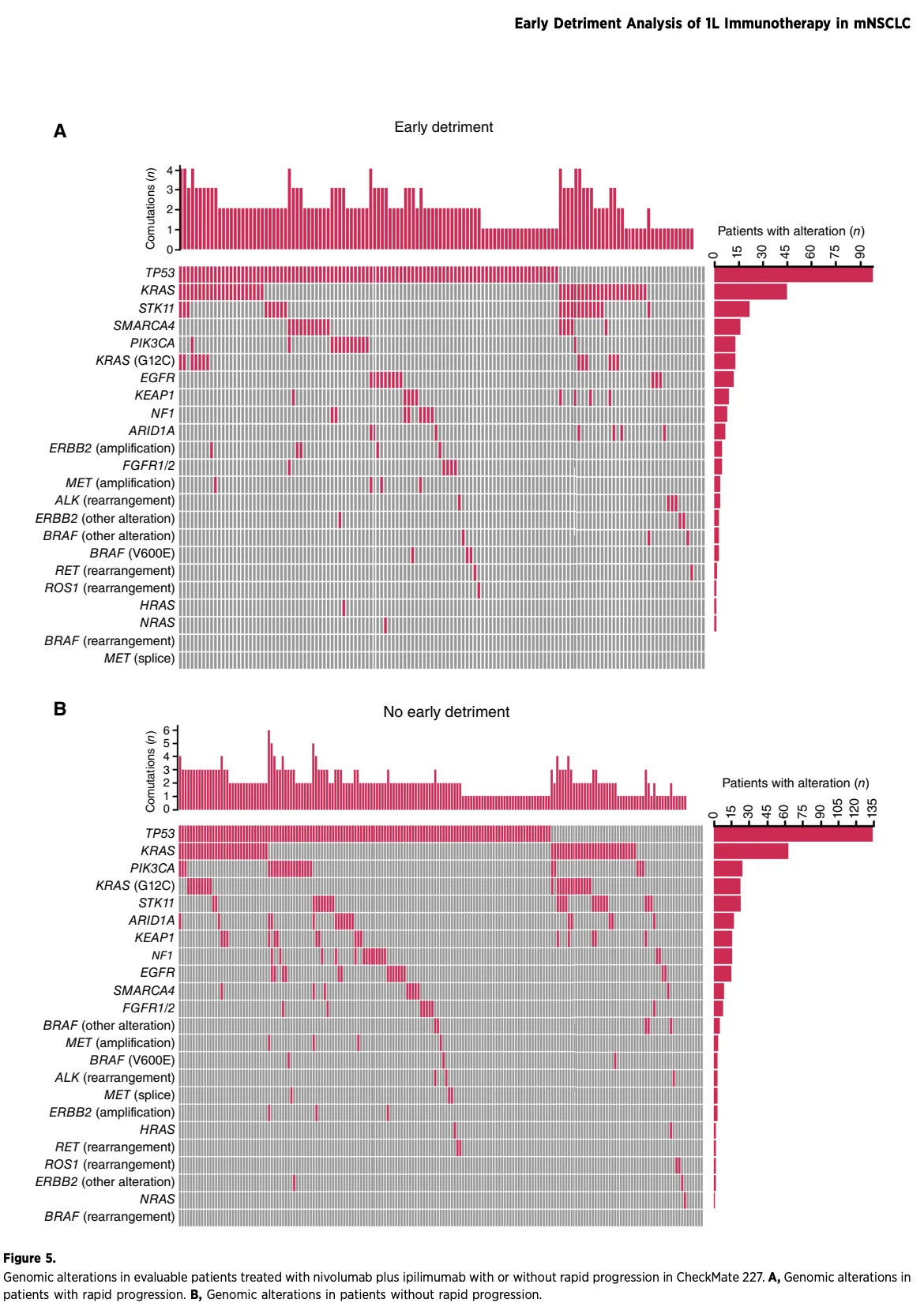
What About STK11 and KRAS?
STK11, TP53, and EGFR alterations were associated with rapid progression in mutation-focused analyses. However, genomic alterations had weaker predictive value than the clinical and laboratory variables in the overall multimodal model.
STK11-mutant disease showed a numerically higher rapid progression rate with nivolumab plus ipilimumab compared with chemotherapy in CheckMate 227. Yet the study was not designed to establish whether STK11, KRAS, or any other individual genomic alteration should determine use of dual immunotherapy.
The results are exploratory and require prospective validation.

What Does This Mean for Clinical Practice?
This analysis does not establish a new biomarker-based algorithm for selecting nivolumab plus ipilimumab or nivolumab plus ipilimumab with chemotherapy.
It does, however, highlight an important clinical reality: some patients with metastatic NSCLC may be at risk of rapid progression with immunotherapy-only treatment, even when long-term benefit is possible for the broader study population.
High neutrophil-to-leukocyte ratio, low TMB, low albumin, low PD-L1 expression, and high monocytic myeloid-derived suppressor cell levels may help identify patients who deserve particularly careful consideration when choosing a first-line regimen.
For patients with a need for rapid disease control, nivolumab plus ipilimumab with limited chemotherapy may offer a strategy that preserves the long-term potential of dual immunotherapy while reducing the early-risk period observed with immunotherapy alone.
The authors emphasize that these data are hypothesis-generating. Prospective studies are needed to determine whether these factors are predictive of benefit from a specific regimen or simply prognostic markers of more aggressive disease.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}