


Tumor mutational burden has become an increasingly important biomarker in oncology, particularly when standard treatment options are limited.
In breast cancer, however, its place remains less clear.
Most breast cancers have a relatively low tumor mutational burden, and only a minority meet the current tumor-agnostic threshold for immunotherapy. Yet a new real-world study suggests that a small group of patients with ultra-high tumor mutational burden, defined as at least 20 mutations per megabase, may represent a clinically meaningful subgroup.
The study found that ultra-high TMB breast cancers were more often estrogen receptor-positive, lobular, and enriched for specific genomic alterations. Among patients with hormone receptor-positive/HER2-negative advanced breast cancer who received single-agent immunotherapy, those with ultra-high TMB had longer time to next treatment, progression-free survival, and real-world overall survival than patients with low TMB.
The results are retrospective and based on a small immunotherapy-treated cohort. Still, they raise an important question: could a TMB threshold of 20 mutations per megabase identify breast cancers more likely to benefit from immune checkpoint blockade?

What Is Ultra-High Tumor Mutational Burden?
Tumor mutational burden, or TMB, measures the number of somatic mutations within a tumor genome.
A higher mutation burden may increase the number of neoantigens that the immune system can recognize, potentially making cancer cells more visible to immune checkpoint inhibitors.
Pembrolizumab already has a tumor-agnostic indication for unresectable or metastatic solid tumors with TMB of at least 10 mutations per megabase, when there are no satisfactory alternative treatment options.
But the threshold of 10 mutations per megabase may not identify all tumors with the same probability of benefit.
Breast cancer is generally considered a low-TMB disease. The present study examined whether tumors with a substantially higher mutation burden, defined as TMB ≥20 mutations per megabase, might have a more distinct clinical and genomic profile.
How Common Was Ultra-High TMB in Breast Cancer?
The genomic cohort included 2,049 patients with clinically advanced breast cancer who underwent comprehensive genomic profiling.
Among them:
- 165 patients, or 8.1%, had TMB ≥10 mutations/Mb
- 45 patients, or 2.2%, had ultra-high TMB ≥20 mutations/Mb
- The median TMB in the ultra-high group was 26.3 mutations/Mb, compared with 2.5 mutations/Mb in tumors with TMB below 20 mutations/Mb.
This confirms that ultra-high TMB breast cancer is rare.
But rare does not mean clinically unimportant, especially when the biomarker may identify an FDA-approved therapeutic option for patients whose disease has progressed after several prior treatments.
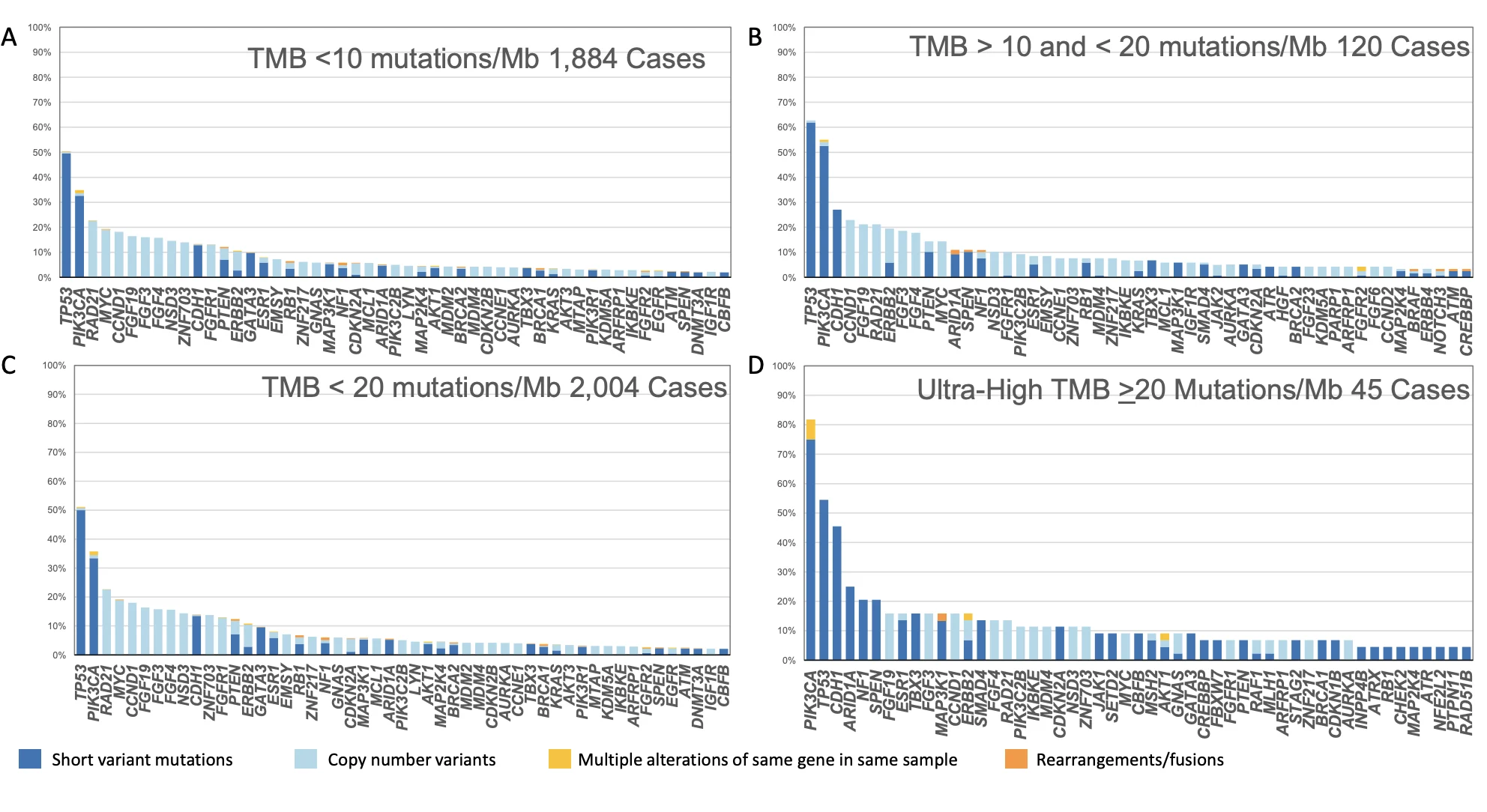
What Did Ultra-High TMB Breast Cancers Look Like?
Ultra-high TMB breast cancers were not randomly distributed across clinical subtypes.
Compared with tumors with TMB below 20 mutations/Mb, ultra-high TMB tumors were more likely to be:
- Estrogen receptor-positive: 86.6% versus 68.2%
- Invasive lobular carcinoma: 40.0% versus 14.5%
- PIK3CA-mutated: 81.8% versus 37.9%
- CDH1-altered: 45.5% versus 12.3%
- APOBEC signature-positive: 82.5% versus 60.3%
- MSI-high: 11.6% versus 0.4%
They also had higher rates of alterations in ARID1A, MAP3K1, NF1, and CDKN2A.
The association with lobular histology and CDH1 alterations is particularly notable. CDH1 loss is a defining molecular feature of many invasive lobular cancers, and the findings suggest that a subgroup of lobular tumors may carry a more complex genomic landscape than usually expected.
Importantly, ultra-high TMB was not associated with significantly higher PD-L1 expression. This reinforces the fact that TMB and PD-L1 reflect different aspects of tumor immunobiology.
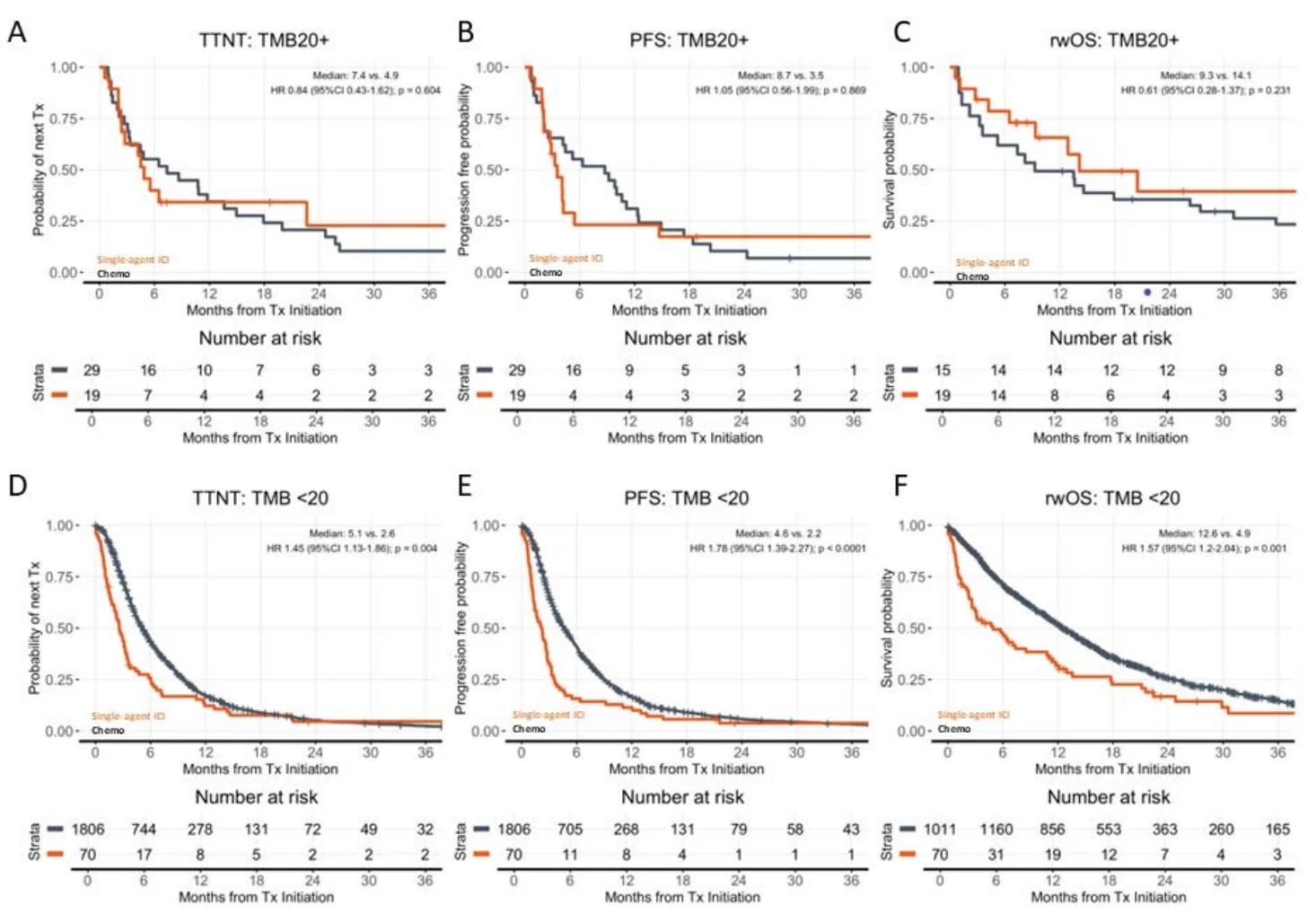
Did Ultra-High TMB Predict Better Outcomes With Immunotherapy?
The clinical outcomes analysis focused on patients with hormone receptor-positive/HER2-negative clinically advanced breast cancer.
Among patients receiving single-agent immunotherapy, 19 had ultra-high TMB and 70 had TMB below 20 mutations/Mb. Most received pembrolizumab, often in later lines of treatment.
Patients with ultra-high TMB had longer outcomes with immunotherapy:
- Median time to next treatment: 4.9 months versus 2.6 months
- Median progression-free survival: 3.5 months versus 1.7 months
- Median real-world overall survival: 14.1 months versus 3.2 months
The real-world overall survival difference was particularly striking, with a hazard ratio of 0.37 for ultra-high TMB compared with TMB below 10 mutations/Mb.
This does not mean that every patient with ultra-high TMB will respond to immunotherapy. The median progression-free survival remained modest, underlining that this is not a universally effective strategy.
However, the longer survival outcomes suggest that ultra-high TMB may enrich for a subgroup capable of deriving meaningful and sometimes durable benefit from single-agent immune checkpoint inhibition.

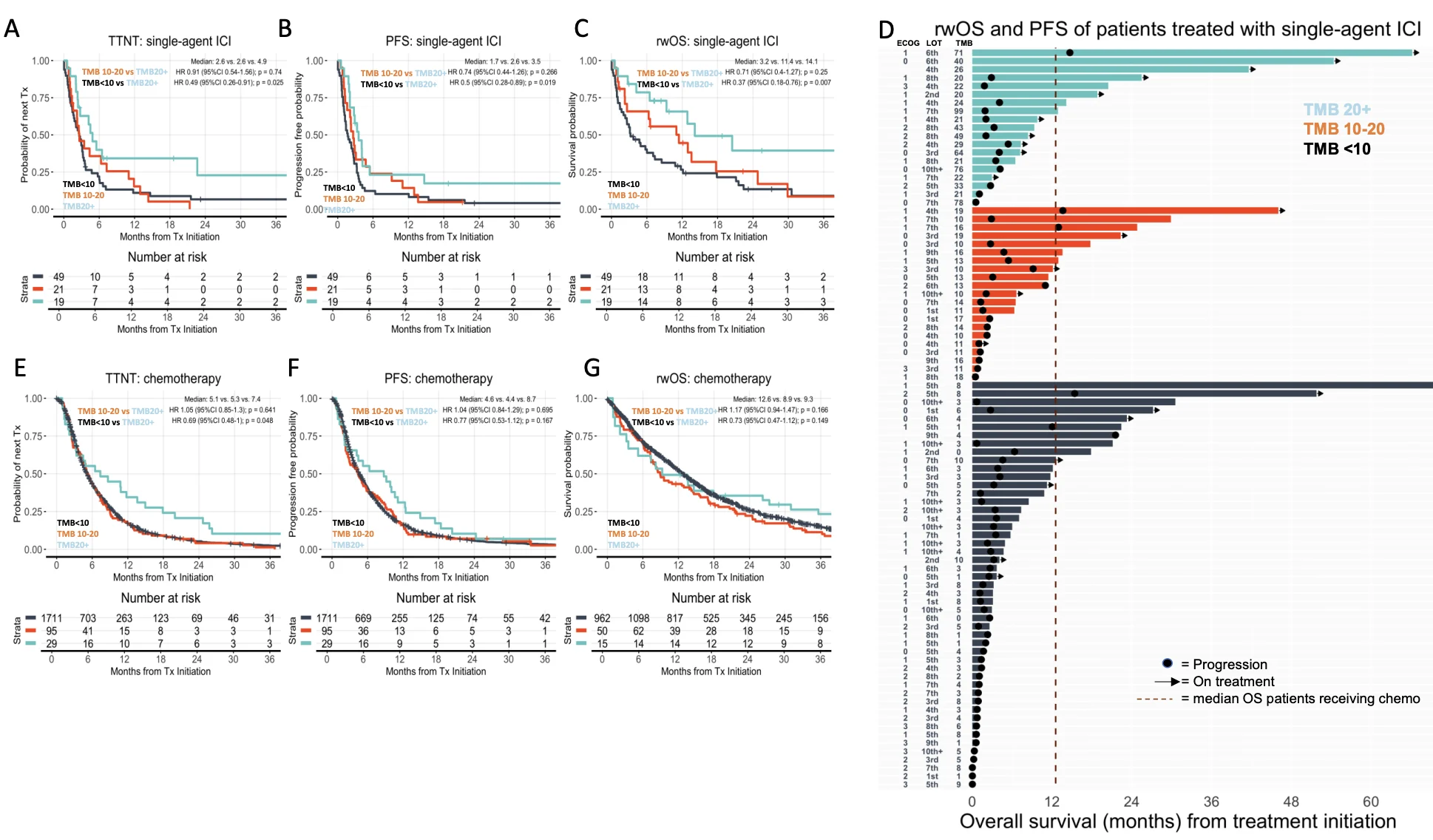
Was the Same Pattern Seen With Chemotherapy?
Notably, the survival advantage was not observed in patients treated with chemotherapy.
Patients with ultra-high TMB who received chemotherapy had a somewhat longer median time to next treatment than those with lower TMB. However, there was no statistically significant difference in progression-free survival or real-world overall survival.
This finding is important because it suggests ultra-high TMB may be predictive of immunotherapy benefit rather than simply a marker of better prognosis.
Still, the study could not fully prove that immunotherapy was superior to chemotherapy within the ultra-high TMB subgroup.
The number of patients was small, treatment assignment was not randomized, and the immunotherapy-treated population had differences in performance status, treatment line, and clinical characteristics that could not be fully balanced.
Why Could This Matter in ER-Positive Metastatic Breast Cancer?
Immune checkpoint inhibitors are already established in selected triple-negative breast cancers, particularly in PD-L1-positive disease.
Their role in hormone receptor-positive breast cancer is much more limited.
Yet the current study shows that ultra-high TMB was more frequent in estrogen receptor-positive disease than in lower-TMB breast cancers. This means a biomarker-driven opportunity may exist in a group not routinely associated with immunotherapy.
For a patient with heavily pretreated ER-positive/HER2-negative metastatic breast cancer, comprehensive genomic profiling may reveal more than targetable mutations. It may identify ultra-high TMB or MSI-high status, creating a potential path toward pembrolizumab.
What Are the Limits of the Evidence?
This was a retrospective, real-world analysis rather than a randomized clinical trial.
Only 19 patients with ultra-high TMB received single-agent immunotherapy. The analysis also relied on electronic health record-derived outcomes, and the investigators could not fully adjust for all treatment-selection factors.
The paper is also an article-in-press version, meaning it may undergo further editorial changes before final publication.
Therefore, these findings should be viewed as hypothesis-generating rather than practice-changing.

The Bottom Line
Ultra-high TMB breast cancer is rare, accounting for about 2% of clinically advanced cases in this analysis.
But this subgroup may be clinically important.
Ultra-high TMB tumors were enriched for estrogen receptor-positive disease, lobular histology, APOBEC mutagenesis, PIK3CA mutation, and CDH1 alteration. In patients with hormone receptor-positive/HER2-negative advanced breast cancer, ultra-high TMB was associated with longer real-world outcomes on single-agent immunotherapy than lower TMB.
The study does not establish a new standard of care. It does, however, support careful attention to TMB values rather than treating every result above 10 mutations/Mb as biologically equivalent.
For some patients, the number may matter more than previously recognized.
{kind=link}
{kind=link}
{kind=link}