


For years, HER2 divided breast cancer into two groups: positive and negative.
Then antibody–drug conjugates began to challenge that boundary.
HER2-low disease entered the treatment conversation. Tumors once considered outside the reach of HER2-targeted therapy became candidates for a new generation of drugs designed to use even modest HER2 expression as a pathway for delivering chemotherapy into cancer cells.
Now, a first-in-human study of trastuzumab brengitecan, known as T-Bren or BL-M07D1, adds another early signal to this evolving story.
In a multicentre phase 1a/1b trial, T-Bren produced objective responses in heavily pretreated patients with HER2-positive, hormone receptor-positive/HER2-low, and hormone receptor-negative/HER2-low advanced breast cancer.
The response rates were striking. The safety profile was also demanding.

What Is T-Bren?
T-Bren is a HER2-directed antibody–drug conjugate, or ADC.
It combines an anti-HER2 antibody with a cathepsin B-cleavable linker and a potent topoisomerase I inhibitor payload called Ed-04. The ADC has a drug-to-antibody ratio of eight.
The design aims to use HER2 as a delivery address. Once the ADC binds to HER2-expressing cancer cells, the payload is released and damages tumor DNA.
This approach may be relevant not only in HER2-positive disease, but also in tumors with lower or uneven HER2 expression, where a bystander effect could potentially extend cytotoxic activity beyond cells with the highest HER2 levels.
How Was the Study Conducted?
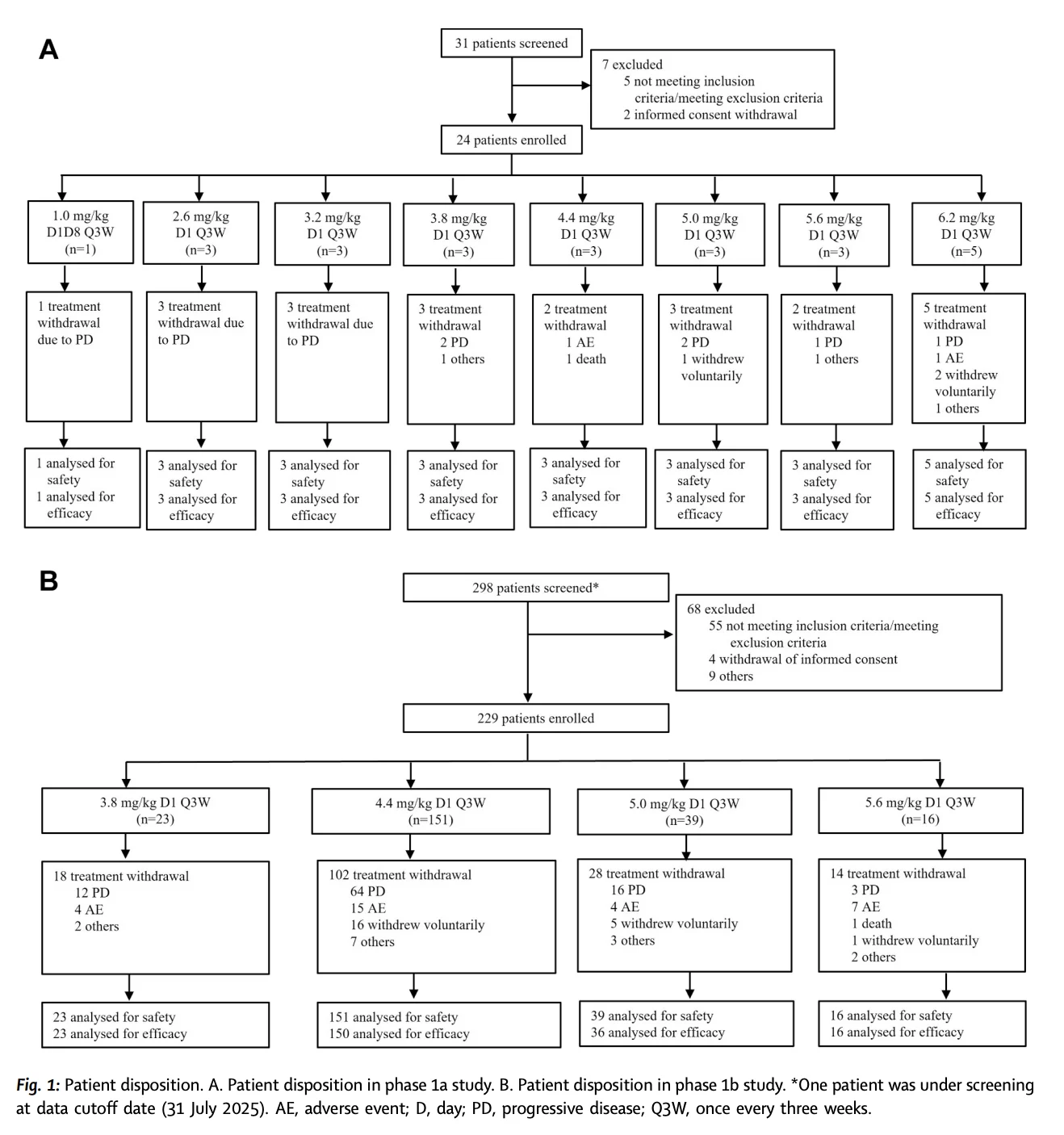
The phase 1 trial enrolled patients with inoperable locally advanced or metastatic breast cancer and other solid tumors across 12 centers in China.
A total of 253 patients received T-Bren between August 2022 and July 2025. Of these, 181 patients had breast cancer.
The trial included dose escalation followed by dose expansion. The expansion phase evaluated doses of 3.8 mg/kg, 4.4 mg/kg, 5.0 mg/kg, and 5.6 mg/kg every three weeks.
Dose-limiting toxicities emerged at 6.2 mg/kg every three weeks. These included grade 4 neutropenia with myelosuppression, grade 3 thrombocytopenia, and grade 4 febrile neutropenia.
The investigators selected 4.4 mg/kg every three weeks as the recommended phase 2 dose for breast cancer.
What Happened in HER2-Positive Breast Cancer?
Among 81 patients with HER2-positive advanced breast cancer, T-Bren achieved an objective response rate of 81.5%.
This included:
- 6 complete responses
- 60 partial responses
- A confirmed objective response rate of 76.5%
- A disease control rate of 97.5%
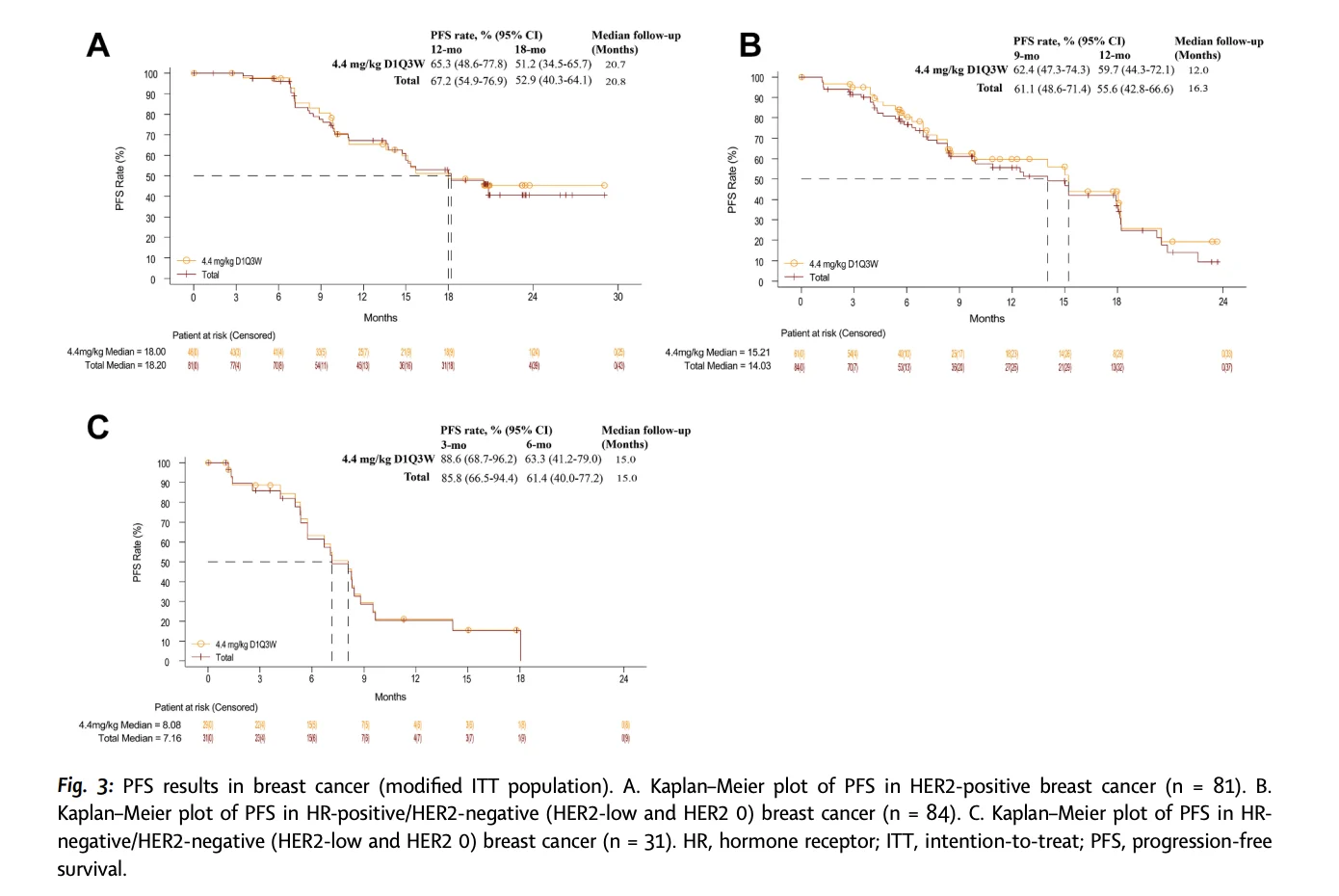
- At a median follow-up of 20.8 months, median progression-free survival was 18.2 months.
The 12-month progression-free survival rate was 67.2%, while the 18-month rate was 52.9%.
In the 4.4 mg/kg cohort, the objective response rate reached 84.8% and the confirmed response rate was 80.4%.
These results were observed in a heavily pretreated population. The median number of prior systemic therapy lines in the HER2-positive breast cancer cohort was three.
That context matters. The data are encouraging, but this was a single-arm phase 1 study and cannot establish how T-Bren compares with current HER2-directed ADCs or other later-line treatment options.

Could T-Bren Extend Benefit Into HER2-Low Disease?
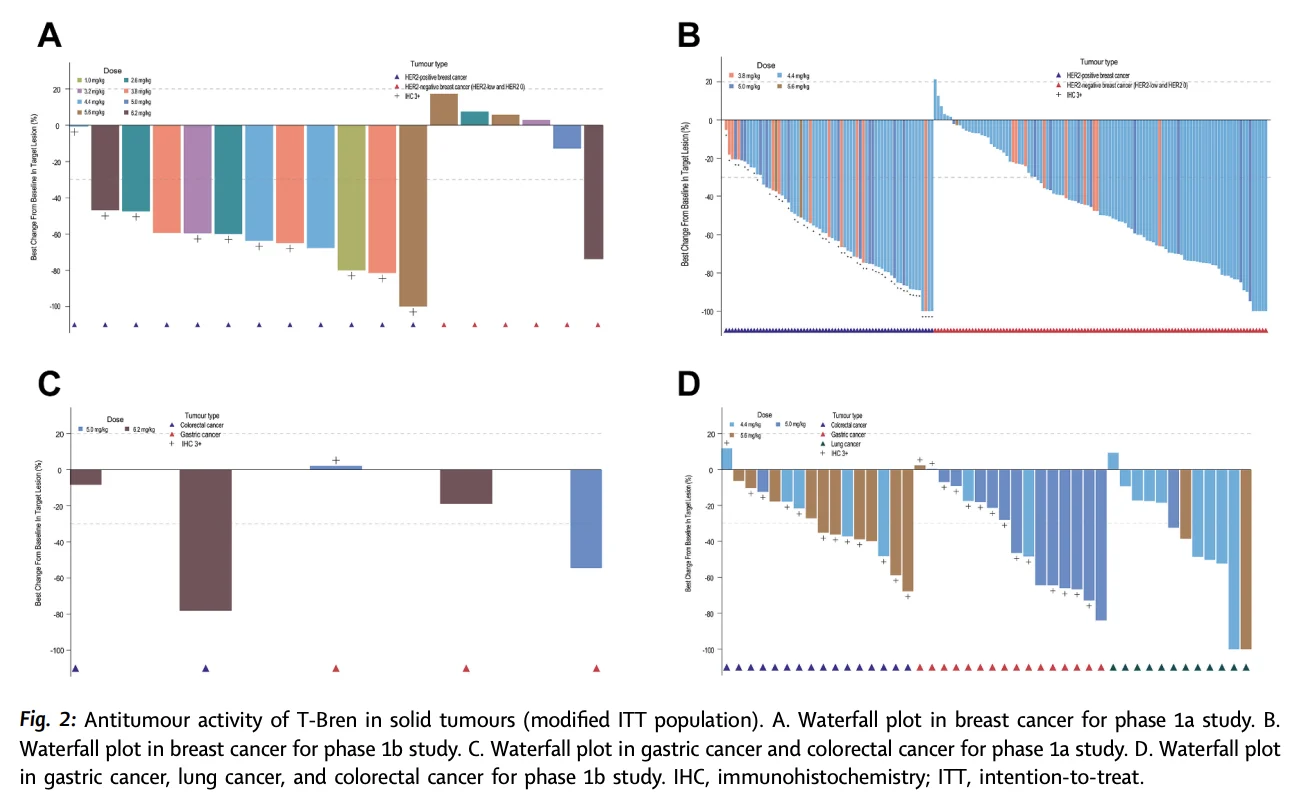
The most intriguing part of the study may be the activity seen beyond conventionally HER2-positive disease.
Among 82 patients with hormone receptor-positive/HER2-low breast cancer, the objective response rate was 69.5%. The confirmed response rate was 67.1%.
Median progression-free survival in this group was 14.0 months.
At the recommended phase 2 dose of 4.4 mg/kg every three weeks, both the objective response rate and confirmed response rate were 72.9%.
The hormone receptor-negative/HER2-low cohort was smaller, including 24 patients. Here, T-Bren achieved an objective response rate of 58.3%.
Three patients achieved a complete response, representing 12.5% of the subgroup.
Median progression-free survival was 7.2 months.
At the 4.4 mg/kg dose, the objective response rate was 63.6%.
These results support the growing idea that HER2 is not simply present or absent. It exists along a continuum, and the right ADC may be able to exploit lower levels of HER2 expression.
The Safety Profile Cannot Be Overlooked
The treatment was active, but it was not a low-toxicity regimen.
Hematologic adverse events were the dominant safety concern.
Across the dose-expansion cohorts, grade 3 or higher treatment-related adverse events included:
- Anaemia: 54.6%
- Neutropenia: 48.5%
- Leukopenia: 41.9%
- Thrombocytopenia: 40.6%
- Serious treatment-related adverse events occurred in 48.5% of patients during dose expansion.
Treatment discontinuation due to treatment-related adverse events occurred in 8.7% of patients, with thrombocytopenia the most common reason.
Interstitial lung disease occurred in 2.6% of patients in the expansion cohorts. Grade 3 or higher pneumonitis was reported in 1.7%.
Two treatment-related deaths due to pneumonia occurred during dose expansion.
The investigators reported that many toxicities could be addressed with dose interruptions, dose reductions, and supportive care. However, the frequency of severe hematologic toxicity will remain a central issue as T-Bren moves into later-stage development.
Why Does This Matter for the HER2 ADC Landscape?
T-Bren enters an increasingly crowded HER2 ADC field.
The challenge for every new ADC is no longer simply to show responses. It must demonstrate where it fits.
Can it deliver longer disease control? Can it remain active in patients previously treated with other HER2-targeted ADCs? Can its toxicities be managed more effectively? Can it offer meaningful activity in HER2-low disease or in patients with brain metastases?
This phase 1 study begins to address the first question: does T-Bren have antitumor activity across a broad HER2 expression range?
The answer appears to be yes.
But the other questions remain open.
The trial was single-arm, non-randomized, and conducted in a Chinese population. Overall survival data are immature. The study also excluded patients previously treated with a topoisomerase I inhibitor-based ADC in the expansion phase, limiting conclusions about use after prior trastuzumab deruxtecan.

What Comes Next?
T-Bren is already moving into further development.
Ongoing studies are evaluating the ADC in HER2-positive breast cancer, HER2-low breast cancer, HER2-expressing gynecologic and urinary tumors, and HER2-mutant non-small cell lung cancer.
Phase 3 studies have also been initiated in advanced HER2-positive and HER2-low breast cancer, as well as in adjuvant HER2-positive disease.
For now, T-Bren remains an investigational therapy.
But its early results highlight the next chapter of HER2-directed treatment: a future in which the HER2 spectrum may matter as much as the HER2 label.
{kind=link}
{kind=link}
{kind=link}