


Tyler Seibert, Assistant Professor in the Division of Radiation Oncology and a member of the RMAS Center for Precision Radiation Medicine (CPRM), shared a post on X:
“Brief. How common is failure of modern active surveillance (AS) for Prostate Cancer (PCa)? Which patients are at higher risk?
Spoiler: it’s pretty simple.
Title: Predicting Active Surveillance Failure for Patients with Prostate Cancer in the Magnetic Resonance Imaging Era: A Multicentre Transatlantic Cohort Study
Authors: Nikita Sushentsev, Irene G. Li, George Xu, Anne Y. Warren, Celeste Y. Hsu, Madison Baxter, Dev Panchal, Christof Kastner, Sean Fernando, Ekaterina Pazukhina, Oleg Blyuss, Alexey Zaikin, Ahmed Shabaik, Anders M. Dale, Michael Liss, Tristan Barrett, Tyler M. Seibert
Read the Full Article.

Issue for AS is choice of endpoint
“Progression” of GG1→GG2 is not meaningful. And progression to GG3 not necessarily a failure of AS, more an indication ⏳for RP/RT
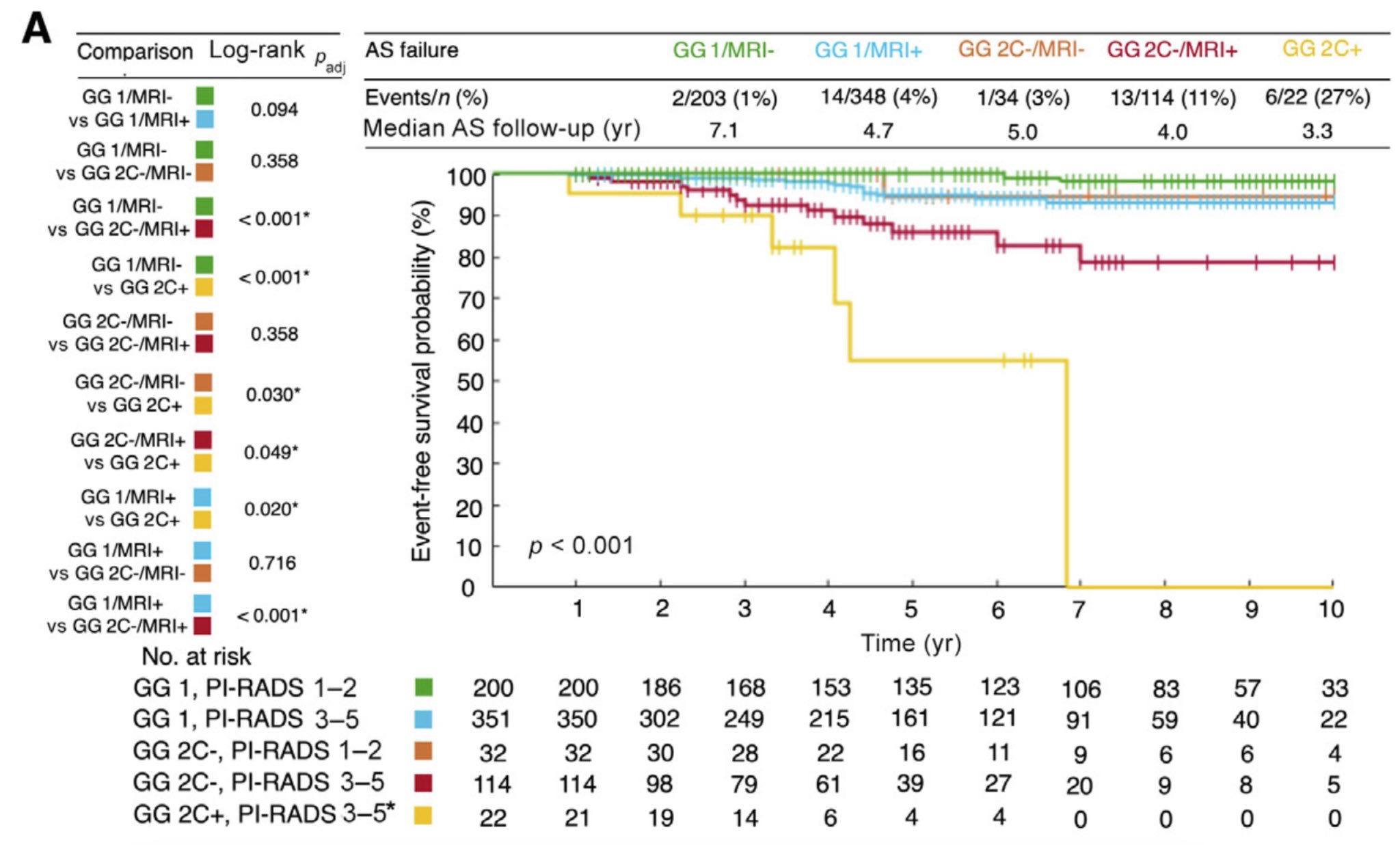
AS failure = any of: N1, M1, GG 4-5, BCR, death from PCa

Many pts on AS for PCa eventually choose radical treatment (RP/RT) even if still eligible for AS. And RP/RT alters the natural history We tackled this via survival analysis If RP/RT w/o failure, we continued to follow pt to see if they later (ever) met AS failure criteria.
Idea is pt on AS and then ever has N1, M1, etc was treated “too late” – had we known, we would have tried for cure earlier
Never experienced AS failure criteria → censor at time of RP/RT
Eventually developed AS failure criteria → count event at time of RP/RT.
We included 799 pts on modern, MRI-driven AS across 3 centers. Two key features explain nearly all risk of AS failure in multivar analysis:
- Cribriform morphology → HR 13
2. PI-RADS 3-5 → HR 5

Summary
AS very safe for all GG1
AS very safe for MRI-invisible GG2 non-cribriform
Cribriform → do not offer AS
MRI-visible, non-cribriform GG2 → AS safe but could benefit from AS intensity?

Open Qs:
- Can we tailor AS intensity based on risk of AS failure?
- Is MRI visibility a surrogate for undetected cribriform morphology?
- Are most non-cribriform GG2 eligible for AS?
- Which post-RP BCRs are real threats?
Thanks to funders, patients, colleagues—especially amazing co-1st authors Nikita Sushentsev, Irene Li, George Xu
AS is critical to early detection to prevent Prostate Cancer deaths. We need to optimize eligibility and protocols to minimize burden but still protect those at risk.”
More posts featuring Tyler Seibert.
{kind=link}