


Krishan Jethwa at ,shared on X:
“Rectal Cancer Tweetorial!!
Rectal cancer is a highly heterogeneous disease with rapid evolution in practice.
Let’s review current data to generate a pragmatic, patient-centric, approach to management!
Thank you ASCO for the opportunity!


Pre-operative RT reduces the risk of pelvic recurrence for patients with rectal cancer.
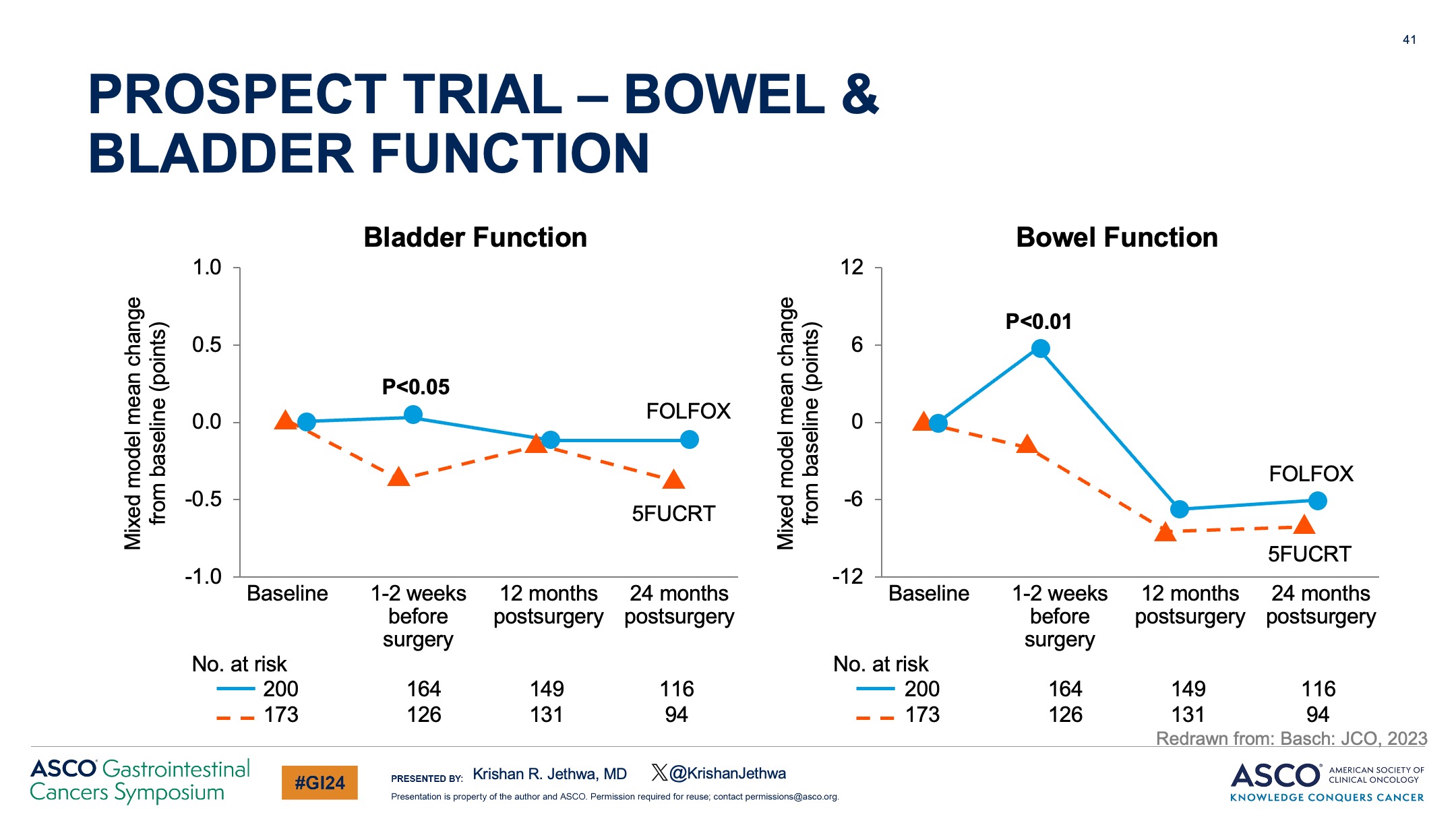
But some patients will suffer from acute and long term toxicity (bladder, bowel, sexual, endocrine dysfunction)
How can we tailor therapy to balance QoL and cancer control?

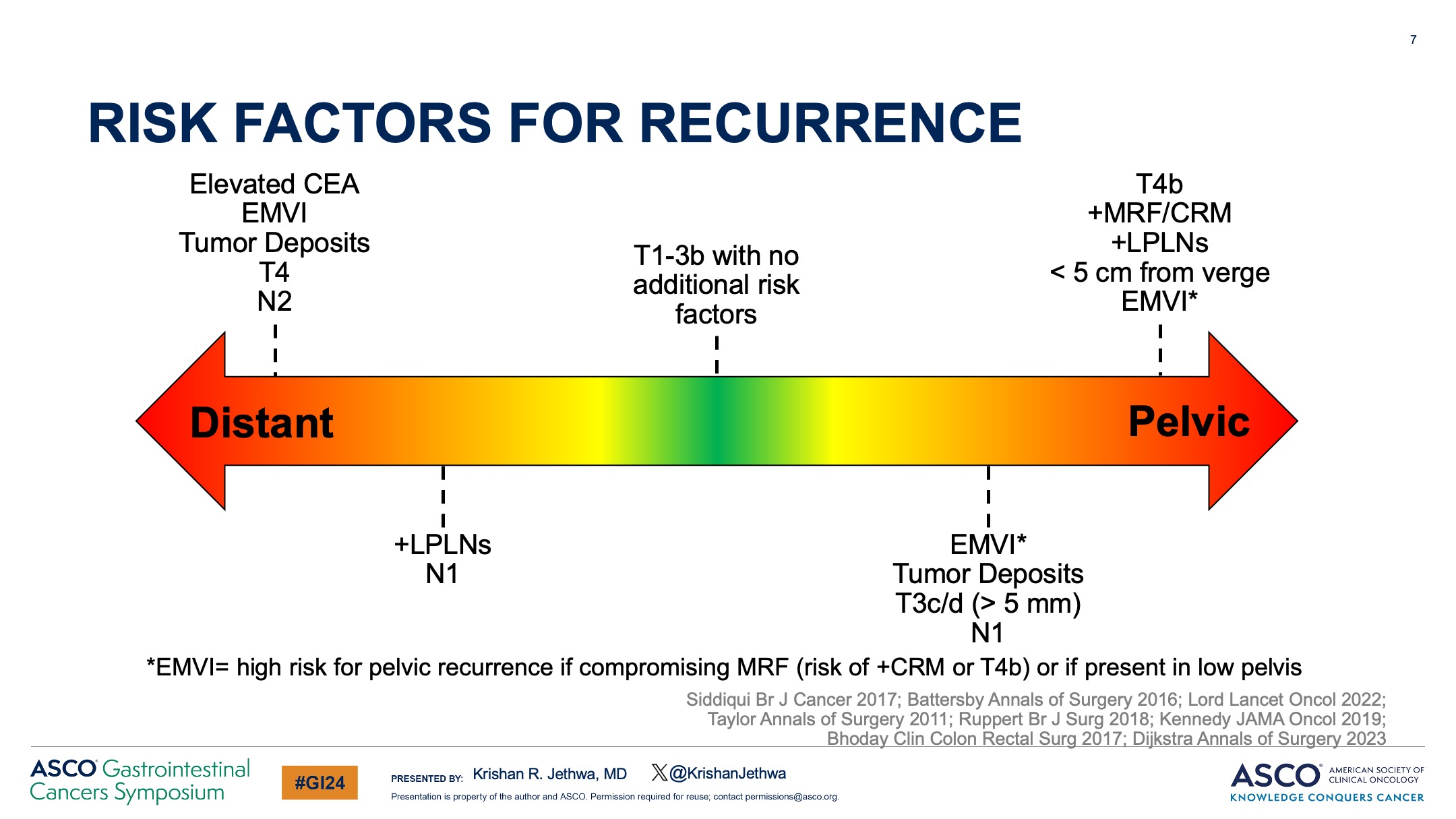
Rectal cancer is highly heterogeneous with a broad spectrum of risk for both pelvic and distant recurrence.
Understanding risk of recurrence is critical in clinical decision making!

Which patients may omit RT?
Mercury, OCUM, and Quicksilver included patients with predominately mid-upper rectal cancers, T2-3bN0, clear MRF, and no EMVI.
Patients treated with up-front surgery Chemotherapy only for pN+ patients.
< 5% + margins
< 5% 5-year pelvic recurrence


For patients with favorable risk cT3N0-1/cT2N1 rectal cancer amenable to LAR, PROSPECT compared:
LC-CRT vs Pre-op chemo +/- selective CRT
Study found no detriment in:
- Local control
- Disease free survival
- Overall survival
BUT pre-op toxicity with FOLFOX.


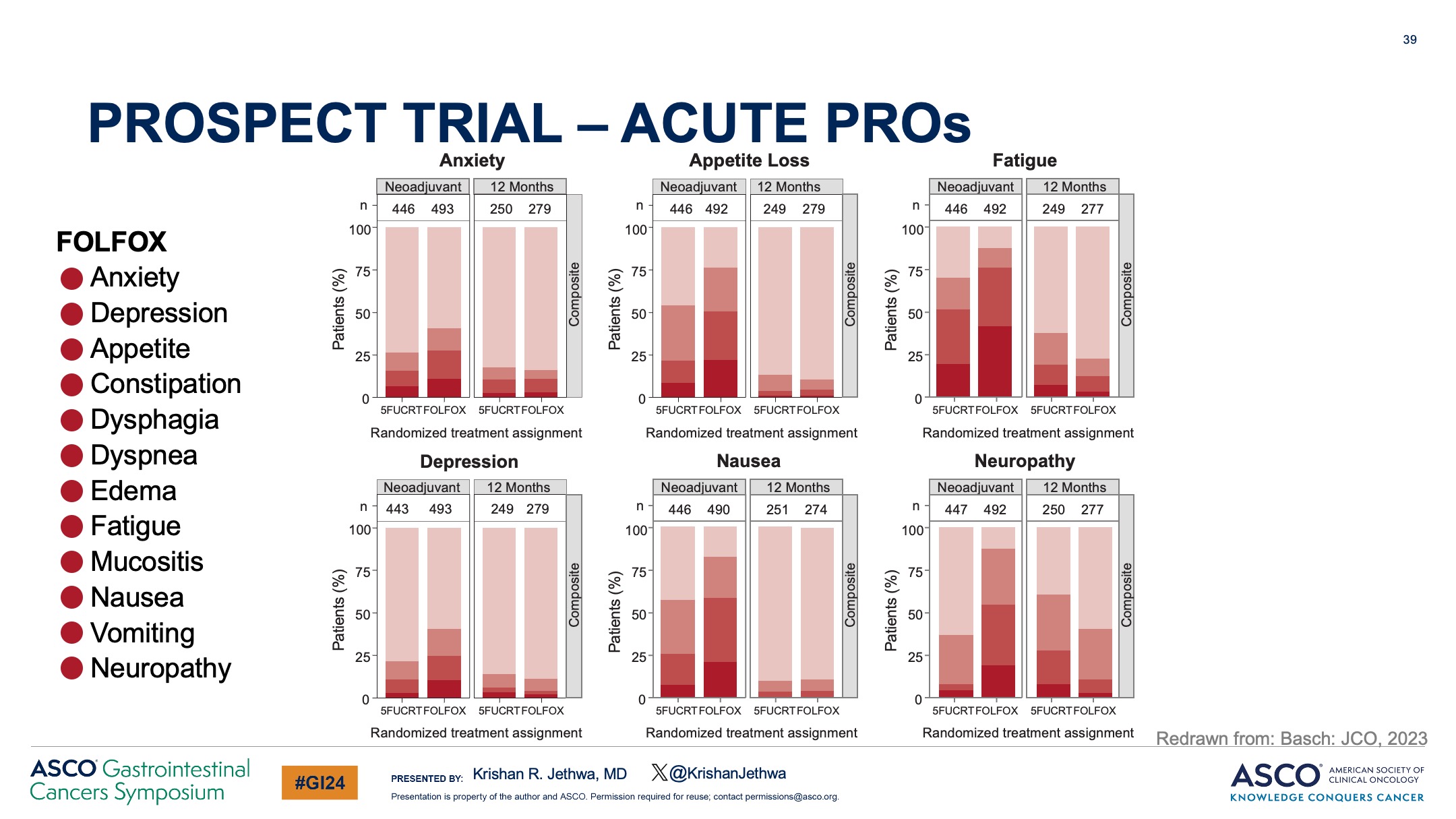
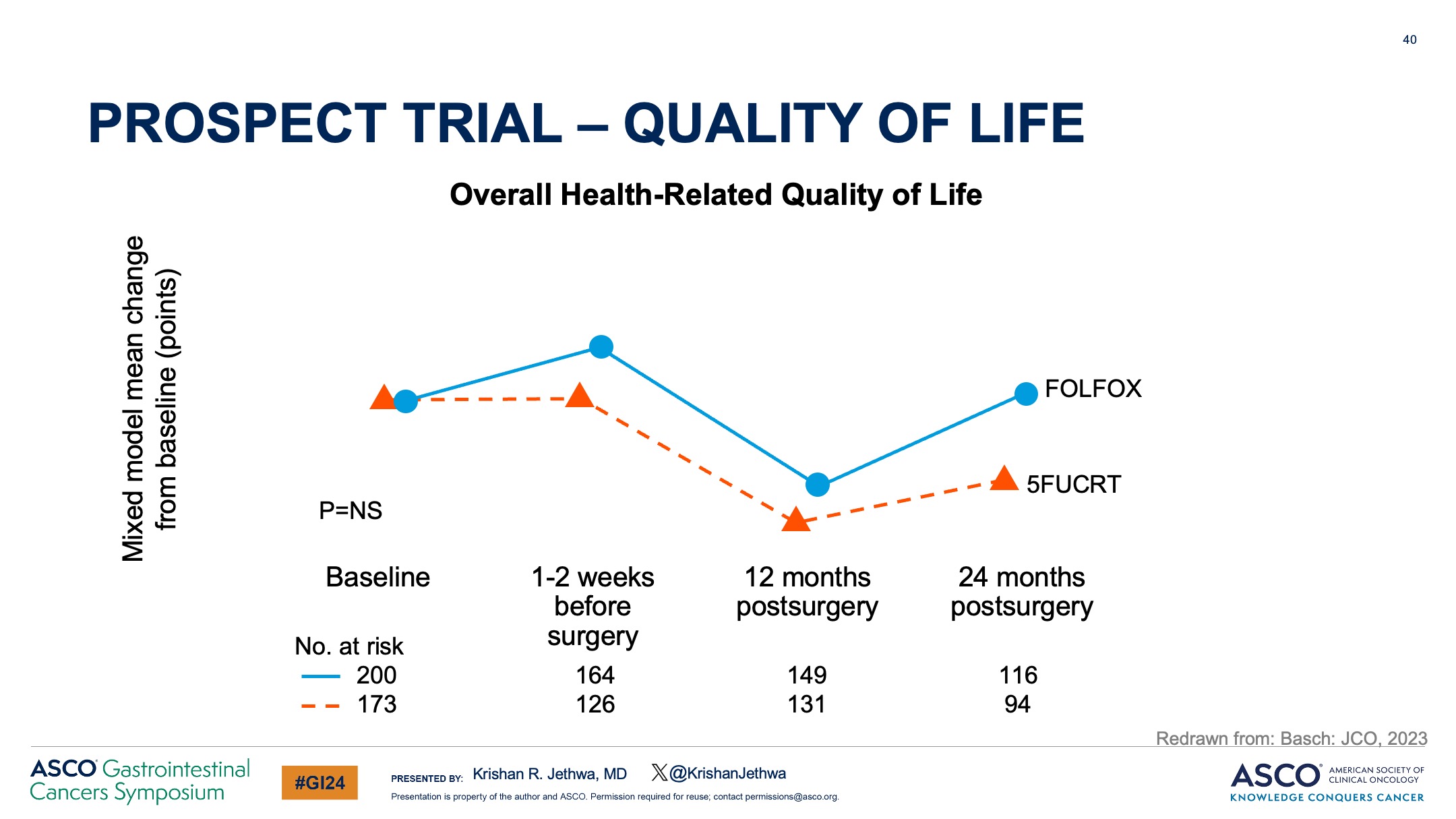
The study included robust collection of PROs which demonstrated:
There were substantial differences in acute PROs favoring CRT but
– No difference in overall QoL
– RT omission did better preserve sexual function

Based upon these data, RT may be safely omitted in patients with favorable risk LARC, including those with:
– Tumors in the mid-upper rectum
– cT2-3
– Clear MRF
– N0-1, limited to the mesorectum
– Planned for surgery with a LAR

What about high-risk rectal cancer?
RAPIDO included patients with T4, cN2, +EMVI, +MRF, or +LPNs.
Randomized:
CRT (Adj chemo optional: 42% received) vs. Intensified TNT regimen of SC-RT – FOLFOX.
Key results improved with TNT:
– Less disease related treatment failure
– Decreased DM


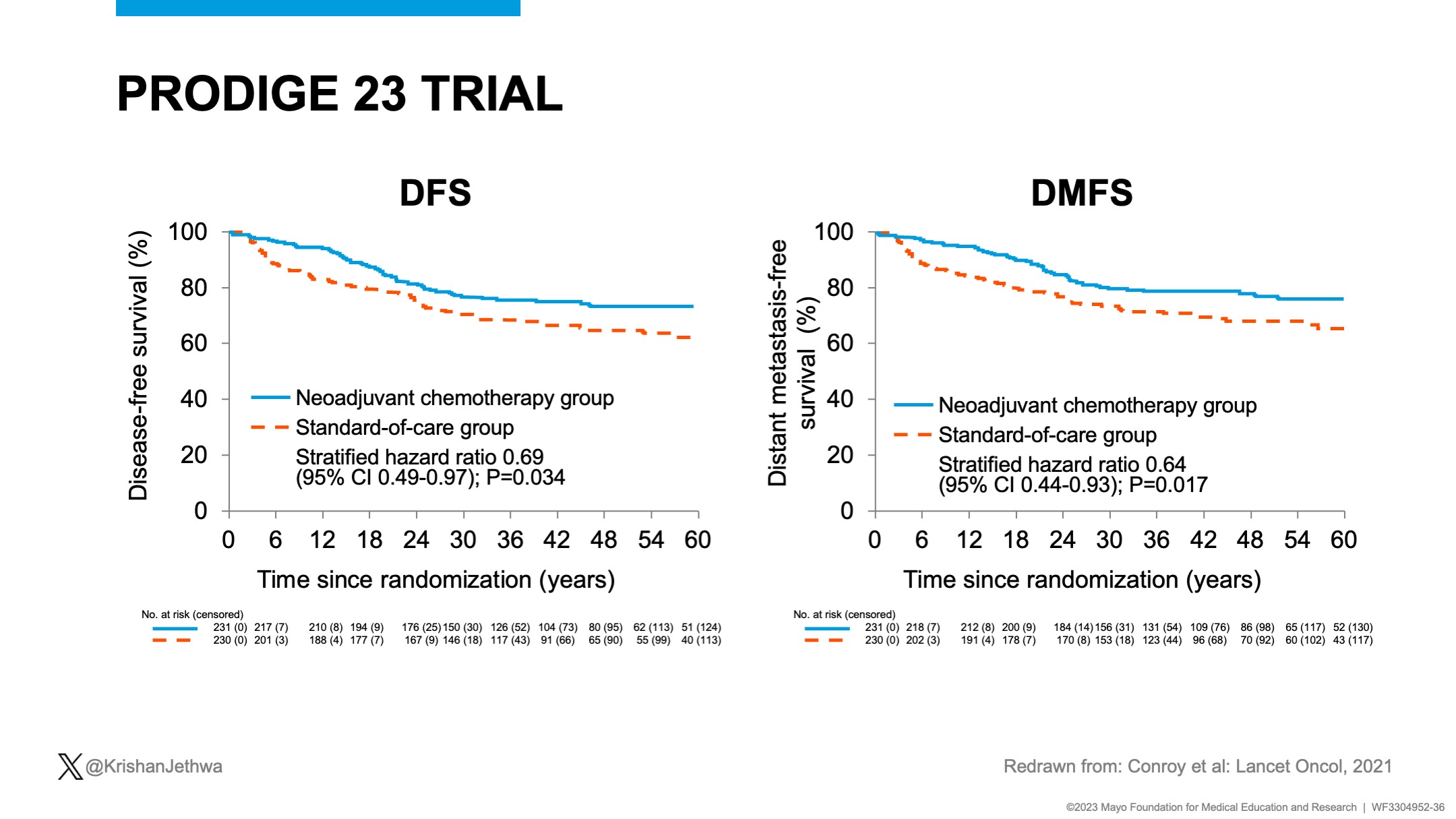
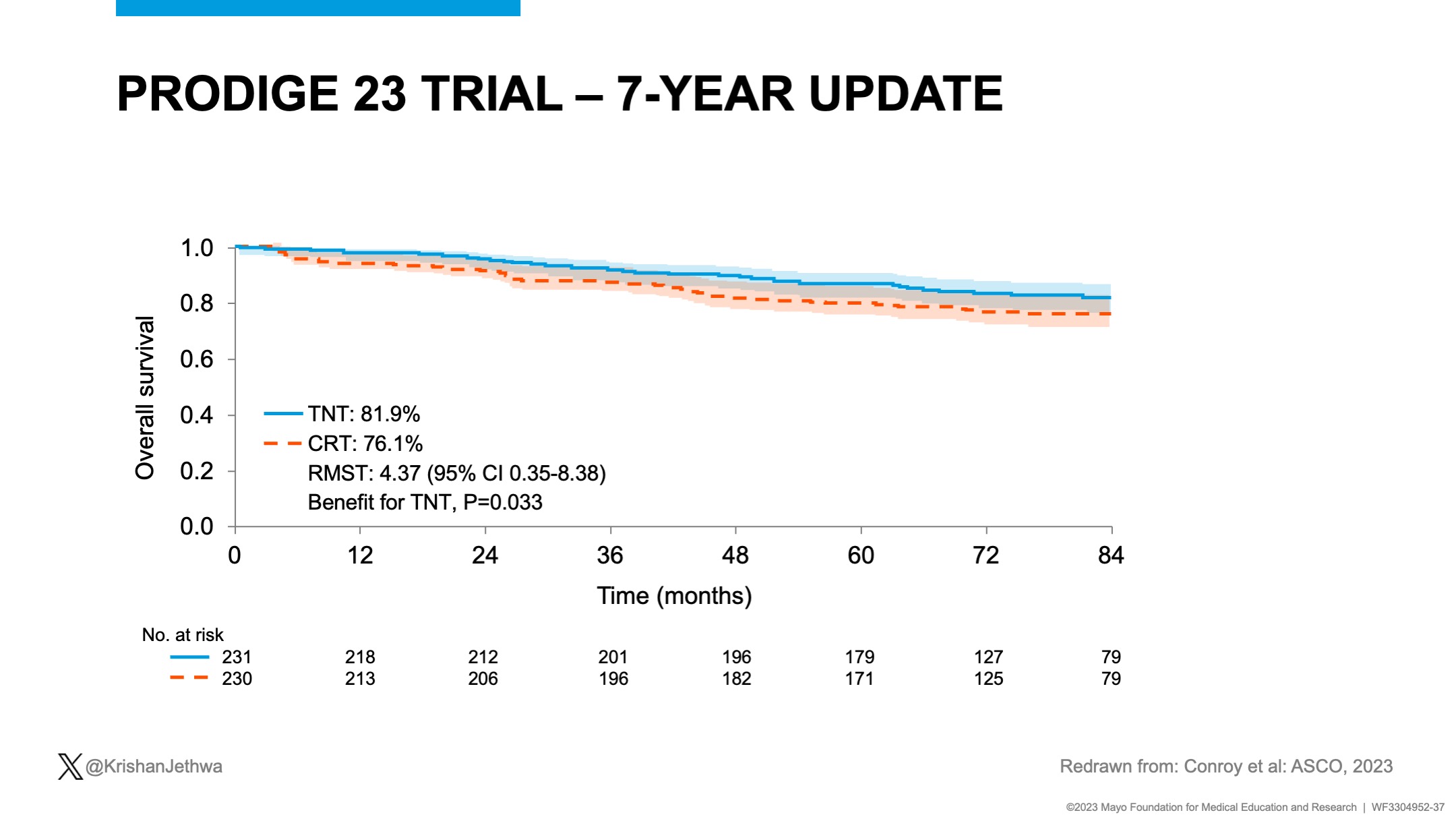
PRODIGE 23 included patients with cT3-4 disease.
Randomized: CRT then FOLFOX vs. mFOLFIRINOX then CRT then S then FOLFOX
Key results improved with TNT!
– Improved DFS
– Decreased DM
– Improved OS!!!

PROSPECT, CONVERT, and FOWARC suggest there is a subset of patients with LARC effectively treated with pre-op FOLFOX without RT
However, these studies had limited representation of high risk disease.
TNT, inclusive of RT, is preferred for patients with high risk disease!


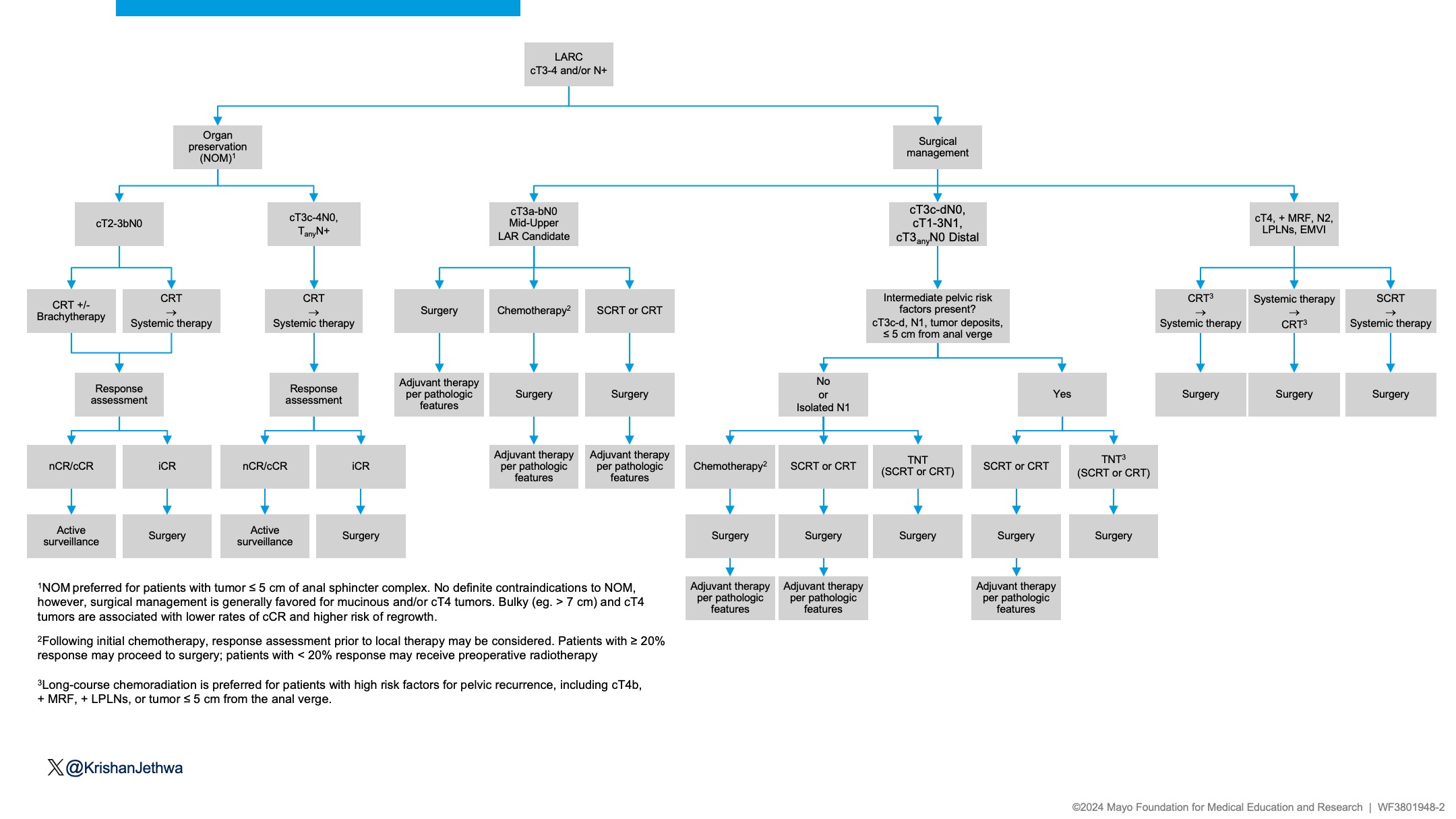
Let’s summarize!
- cT3a-bN0 tumors in the mid-upper rectum amenable to LAR with no additional risk factors – consider RT omission.
- High-risk rectal cancer (cT4, N2, + MRF, LPLNs, EMVI) – TNT


The intermediate risk cohort is much more nuanced!
- Isolated N1, limited to mesorectum
- Consider pre-operative chemotherapy with omission of RT
- Additional pelvic risk factors (T3c-d, tumor deposits, EMVI, distal tumor)
- Favor addition of RT

Let’s discuss SC-RT vs. LC-CRT
SCRT= similar LC, DFS, OS in prior studies of “average risk” patients.
RAPIDO= high risk: higher pelvic recurrence (10% vs. 6%) with SC-TNT vs. LC-CRT.
LC-CRT may be preferred for patients with high-risk rectal cancer.


Organ preservation?
Goal= Preserve QoL and Function
LAR resulting in a low/coloanal anastomosis associated with poor bowel function.
RT + Surgery is associated with poorer function.
- Bowel
- Bladder
- Sexual
Omission of surgery may better preserve function.

Let’s review sequence of therapy!!
OPRA: ~50% may achieve long term organ preservation.
CRT then chemo sequence vs. chemo then CRT: CRT then chemo sequence preferred for NOM.
- Less local regrowth and
- Increased organ preservation with CRT – chemo
- No difference in DFS or DFS after TME (initial iCR or regrowth)

How can we improve cCR and organ preservation?
RT perspective:
OPERA Trial
54 Gy/30 Fx CRT vs. 45 Gy/25 Fx CRT + Brachy boost (90 Gy/3 Fx)
– Brachy= 3-year organ preservation: 81% vs. 59%
– No detriment in severe toxicity or function!
Supports RT dose intensification.

Key conclusions
- RT may be omitted in patients with MRI defined- favorable risk disease
- TNT preferred for high risk disease
- Organ preservation better preserves QoL and function
- CRT then chemo sequence preferred for NOM
LARC Algorithm here!
For discussion!”


Source: Krishan Jethwa/X
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}