


Chokri Ben Lamine, Adult Hematology, Stem Cell Transplantation and Cellular Therapy Assistant Consultant at King Faisal Specialist Hospital and Research Center shared a post on X:
“Key Types of TMA in Pregnancy and Management.
Thrombotic Thrombocytopenic Purpura (TTP):
Cause: Severe ADAMTS13 deficiency (<10%) leading to uncontrolled platelet aggregation.
Diagnosis:
- ADAMTS13 activity <10%.
- ADAMTS13 IgG titers.
- Genetic mutational analysis in congenital TTP (cTTP).
Treatment:
- Immune TTP (iTTP): Plasma exchange (PEX) + corticosteroids.
- Congenital TTP (cTTP): Plasma infusions.
What’s New:
Caplacizumab, a VWF-blocking monoclonal antibody, is now used in refractory iTTP to prevent microthrombi.
HELLP Syndrome (Hemolysis, Elevated Liver Enzymes, Low Platelets):
Cause: Severe endothelial dysfunction due to placental ischemia, leading to hemolysis, liver dysfunction, and thrombocytopenia.
Diagnosis:
- LDH >600 IU/L (hemolysis).
- AST/ALT ≥2x ULN (liver dysfunction).
- Platelet count <100,000.
Treatment:
- Deliver the fetus and placenta as soon as possible.
- Avoid delaying delivery in HELLP as maternal and fetal risks increase rapidly.
What’s New:
- Differentiation from CM-TMA: Use serum creatinine (>1.9 mg/dL) and LDH (>600 IU/L) thresholds.
- Advanced testing like sFlt-1/PIGF ratio may help differentiate HELLP from preeclampsia.
Complement-Mediated TMA (CM-TMA):
Cause: Dysregulation of the complement system due to genetic mutations or autoantibodies (e.g., anti-FH), leading to endothelial damage and platelet activation .
Diagnosis:
- Genetic testing for complement proteins (e.g., C3, CFB mutations).
- Anti-FH antibody titers.
Treatment:
- C5 inhibitors (eculizumab/ravulizumab) block complement activation.
- Plasma exchange is used if C5 inhibitors are unavailable, though efficacy is limited.
What’s New:
- Ravulizumab approved for postpartum CM-TMA.
- Antiphospholipid Syndrome (APS):
Cause: aPL antibodies (LA, aCL, β2GPI) cause endothelial dysfunction and thrombosis.
Diagnosis:
- aPL antibody titers (persistent positivity).
- History of thrombotic or obstetric complications.
Treatment:
- LMWH + aspirin for pregnancy prophylaxis.
- IVIG in recurrent pregnancy losses despite anticoagulation.
What’s New:
- Trials for novel biologics targeting B cells (anti-CD20), BAFF, and complement pathways.
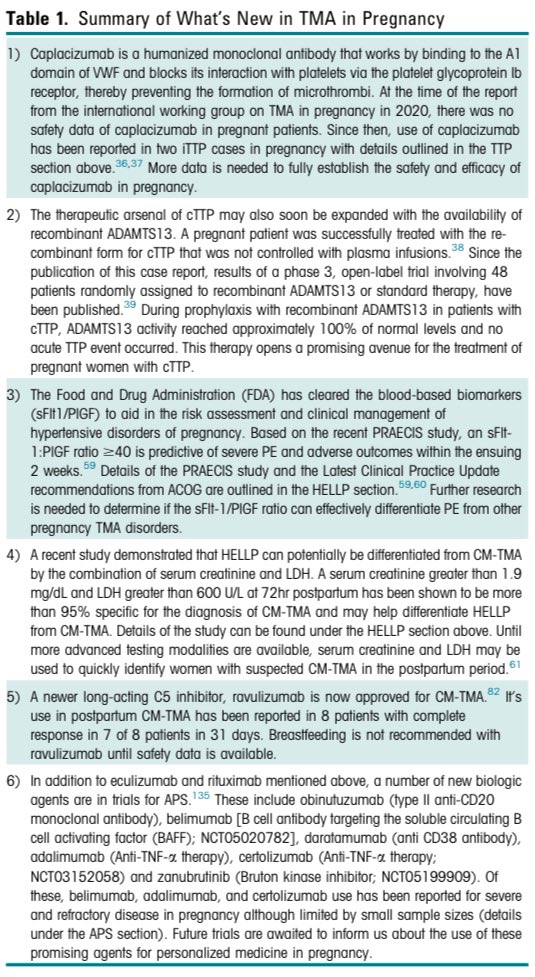
What’s New in TMA in Pregnancy?
Caplacizumab:
- Blocks platelet-VWF interaction, preventing microthrombi in iTTP.
- Refractory cases have shown improvement with its use.
Recombinant ADAMTS13:
- Promising in congenital TTP.
- Achieved near-complete normalization of ADAMTS13 activity during pregnancy trials.
sFlt-1/PIGF Ratio:
- Differentiates preeclampsia from HELLP syndrome or CM-TMA.
- A ratio >40 predicts severe PE and adverse maternal outcomes.
Ravulizumab:
- Long-acting C5 inhibitor now approved for CM-TMA.
- Offers postpartum efficacy in complement-mediated cases.
Novel Biologics:
- Anti-CD20 (obinutuzumab), anti-TNF (adalimumab, certolizumab), and others under investigation for APS and CM-TMA.
Key Differentiators in TMA Types:
- TMA Type Diagnosis Key Treatment.
- TTP ADAMTS13 <10%, IgG titers PEX + steroids.
- HELLP LDH >600, AST/ALT >2x ULN, Platelets <100k Deliver fetus & placenta.
- CM-TMAGenetic testing, Anti-FH antibodies C5 inhibitors or plasma exchange.
- APSaPL antibody titers (LA, aCL, β2GPI) LMWH + aspirin, IVIG for losses.
Key Exam and Clinical Tips:
- TTP: Caplacizumab for refractory cases; know ADAMTS13 criteria.
- HELLP: Immediate delivery is key; delay worsens outcomes.
- CM-TMA: Complement activation = C5 inhibitors like eculizumab/ravulizumab.
- APS: Focus on prevention with LMWH/aspirin during pregnancy.
- Overlap awareness: Distinguish TTP, HELLP, and CM-TMA with lab markers
From:
- Thrombotic Microangiopathy in Pregnancy.
- Current Understanding and Management.
- Strategies by Manuel Urra and al.”


For more updates, follow OncoDaily.
{kind=link}
{kind=link}