


Manni Mohyuddin, Assistant Professor at the Huntsman Cancer Institute at the University of Utah, shared a post on X/Twitter:
”There is a lot of progress that happens every year in myeloma. Learnt a lot in 2023, from both negative and positive trials, and am thankful for the progress. In this post, I will highlight 10 important myeloma publications from 2023 that shaped my thinking and practice.
Each study in this thread was published in 2023. Abstracts/posters not included. I will provide my interpretation with each study. Some nuance may be lost, as I try to fit it within the confines of a tweet. This is not in any particular order. Lets start!
1. Cilta-cel had better PFS than dara/pom/dex for patients with 1-3 prior lines of therapy, all of whom were len-refractory. I am not sure cilta-cel is ‘safer’, but this will be integral to allow earlier access for patients who need it. Read further.
2. The bar was set low, but belantamab could not beat pomalidomide-dexamethasone in a randomized trial. Marginal drug. I do not know solution Balance between having ethical/fair trials versus increased likelihood of failure with head to head design. Read further.
3. In a randomized trial, Dara-RVd/auto/Dara-Len maintenance had better PFS than RVd/auto/len maintenance. I will use quad up-front for fit patients. I will not use dara for maintenance however- this trial doesn’t isolate effect of maintenance. Read further.

4. Ide-cel is clearly not curing patients- although its confirmatory randomized trial was done in a later-line setting compared to cilta-cel. I wish we had graphs like axi-cel for DLBCL- but this curve does not inspire.

5. In a testament to how great daratumumab is- it led to an overall survival advantage in a relapsed/refractory population, even with high rates of cross-over. Use this drug early. It combines well with other drugs, without much increased toxicity. Read further.

6. The only study to make this list that is not a trial. The diagnostic reclassification of myeloma has not aged well. Pts with FLC ratio of >100 do not have a 80% risk of prog in 2 years- the reality is likely ~30% I offer active surveillance. Read further.

7. The most innovative trial of its time-that does not simply add active drug and measure PFS/MRD- the MASTER study. The role of maintenance in era of quads and MRD neg should be questioned- and we owe it to our patients to get rid of maintenance. Read further.

8. In a heavily pre-treated population, mezigdomide+dex demonstrated (some) activity. For patients today who have had disease relapse post BCMA and GRPC5D, I do wish access to this drug was available. Await randomized data. Read further.

9. The OPTIMUM study should be commended for its design and ability to enroll such a high-risk patient population. I still wonder if outcomes would have been the same with less therapy. Useful benchmark for future studies. Read further.
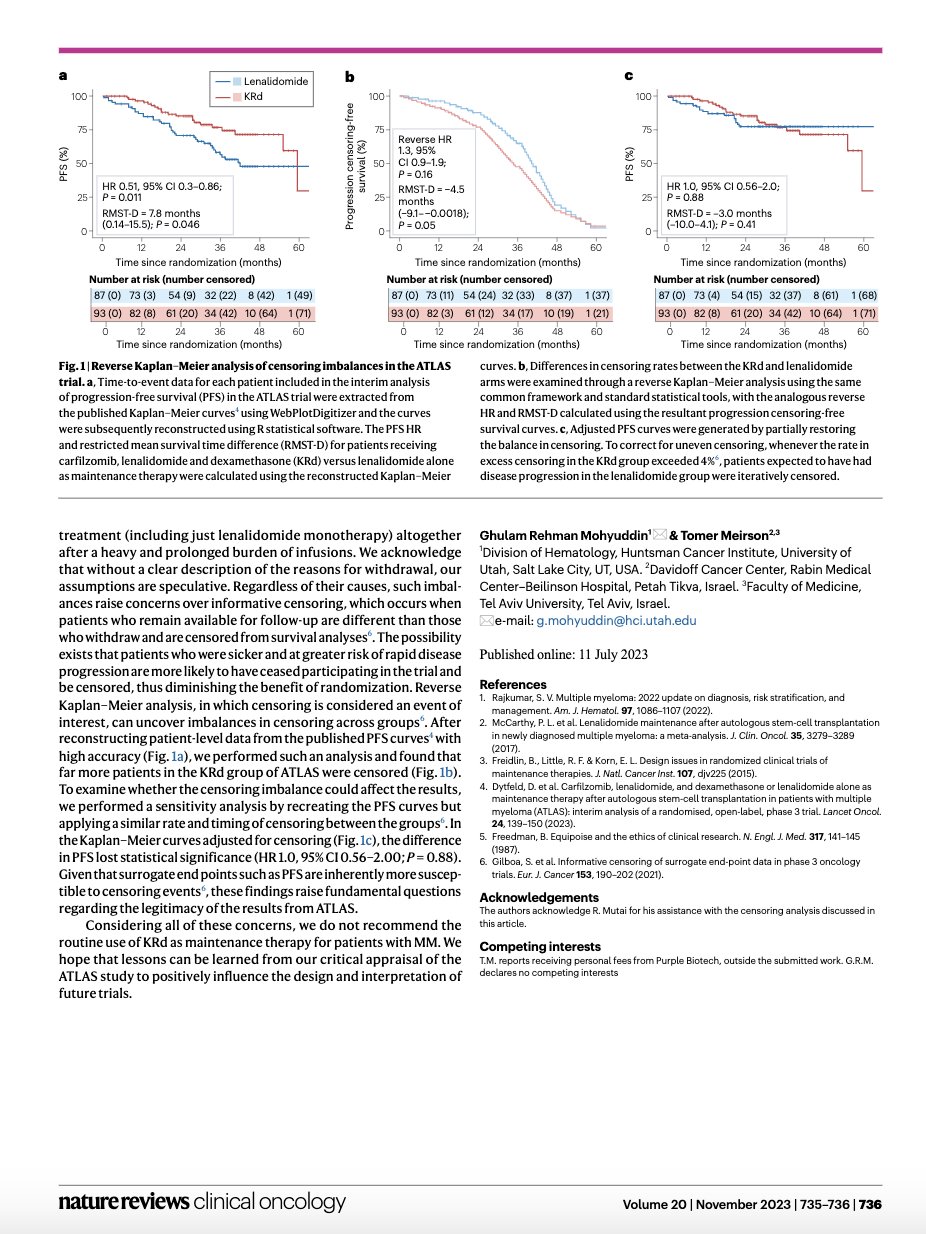
10. There are numerous ways you can prolong a PFS, but prolonged carfilzomib+lenalidomide+dexamethasone maintenance after auto is probably not the best way to do it. Although ATLAS trial higher PFS, widespread censoring/ pt drop-out limit applicability. Read further.

Each of these trials advanced my understanding of myeloma. Thankful for all the progress in this field. Thanks for reading and happy holidays to all! END.”
Source: Manni Mohyuddin/X
{kind=link}