
Miguel Bronchud: Underestimation of Risk by Biopsies Alone Could Lead to Undertreatment in Prostate Cancer
Miguel Bronchud, Co-Founder and Advisory Board at Regenerative Medicine Solutions, shared on LinkedIn about a paper by Neal A. Patel et al. published in JAMA Oncology:
“Prostate cancers are an example of how ‘underestimation of risk’ by biopsies alone could lead to undertreatment and poor outcomes?
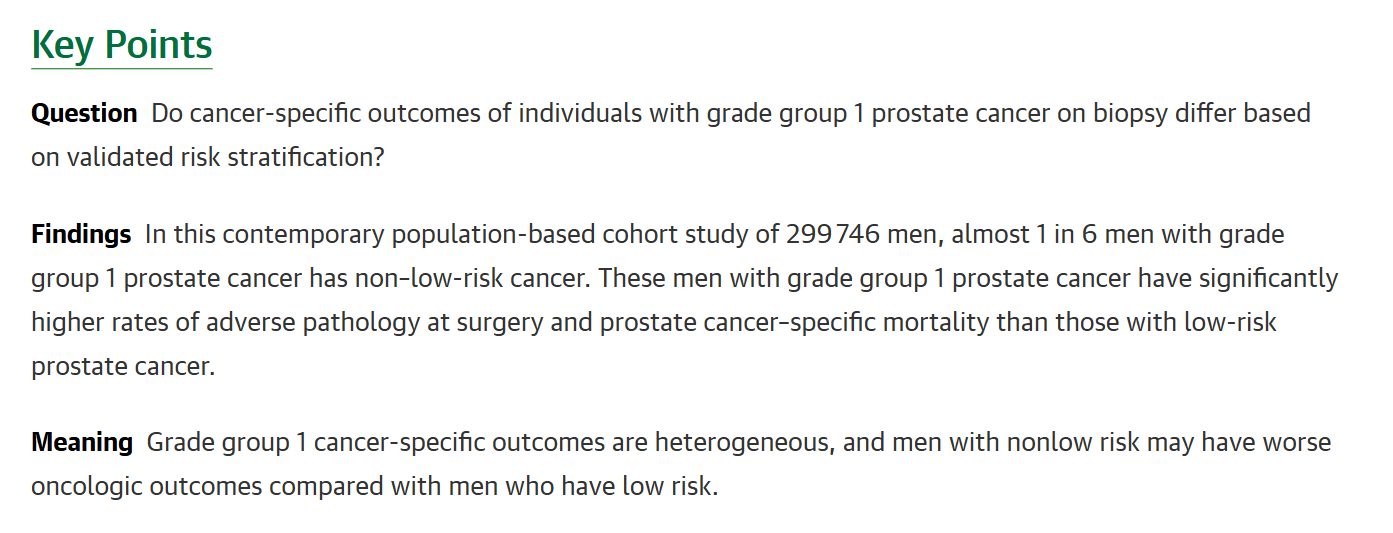
Grade group 1 cancer-specific outcomes are heterogeneous- more meaningful molecular information is required to improve outcomes predicted by histopathology alone? Can liquid biopsies provide useful complementary information?
This cohort study assesses cancer-specific outcomes of localized grade group 1 prostate cancer stratified by risk category. A population-based cohort study using Surveillance, Epidemiology, and End Results data was performed to assess cancer-specific outcomes in 117 162 men with localized GG1 prostate cancer stratified by National Comprehensive Cancer Network risk groups between January 1, 2010, and December 31, 2020.
Competing risk analyses and multivariable regression determined rates of prostate cancer–specific mortality and associations with prostatectomy adverse pathology. Data were analyzed from July 1, 2024, to October 1, 2024.
Main Outcomes: Prostate cancer–specific mortality and risk of adverse pathology at surgery in GG1 prostate cancer.
Results:
Among 117,162 men with biopsy GG1 prostate cancer, 10,440 (9%) had favorable intermediate-risk disease, 3145 (3%) had unfavorable intermediate-risk disease, and 4539 (4%) had high-risk disease. Median age was 64 years (IQR, 58-69 years). A total of 867 men with high-risk GG1 prostate cancer (60%) had adverse pathology at prostatectomy.
The prostate cancer–specific mortality rates for unfavorable intermediate-risk GG1 and for high-risk GG1 were 2.4% and 4.7%, respectively, comparable to the prostate cancer–specific mortality rates for favorable intermediate-risk GG2 and unfavorable intermediate-risk greater than or equal to GG2, which were 2.1% and 4.0%, respectively.
In adjusted analyses, favorable intermediate-risk GG1 (adjusted hazard ratio [AHR], 1.60; 95% CI, 1.30-1.96), unfavorable intermediate-risk GG1 (AHR, 2.10; 95% CI, 1.53-2.89), and high-risk GG1 (AHR, 3.58; 95% CI, 2.93-4.38) were associated with increased risk of prostate cancer–specific mortality compared with low-risk GG1.
Conclusion
Approximately 1 in 6 men with GG1 prostate cancer has intermediate-risk or high-risk disease.
Biopsy GG1 prostate cancer has heterogeneous long-term outcomes that are reflected in adverse pathology and prostate cancer–specific mortality. These data indicate that not all GG1 prostate cancer follows an indolent course.
A subset of men with biopsy GG1 prostate cancer have outcomes comparable to those of men with higher-grade intermediate-risk prostate cancer, a group that often undergoes treatment.
These findings should be considered in the reclassification debate.
‘We don’t want to miss aggressive cancers that initially present as grade group 1 on biopsy. Such underestimation of risk could lead to undertreatment and poor outcomes,’ said at ASCO- Post co-senior author Bashir Al Hussein, MPH, MD, Assistant Professor of Urology and Population Health Sciences at Weill Cornell Medicine; Urologist at NewYork-Presbyterian/Weill Cornell Medical Center; and Member of the Sandra and Edward Meyer Cancer Center at Weill Cornell Medicine.
Classifying tumors by grade group alone based on biopsies may lead to potential underestimation of disease risk and undertreatment.
‘There is a misunderstanding that ‘low grade’ and ‘low risk’ are the same. Here, we show clearly that they are not,’ said co-senior study author Jonathan Shoag, MD, at Case Western Reserve University and Urologist.
See also a previous article.
This observational study uses registry data to compare rates of adverse functional outcomes between specific treatments for localized prostate cancer (radical prostatectomy, external beam radiotherapy, brachytherapy, or active surveillance for favorable-prognosis disease and radical prostatectomy or external beam radiotherapy with androgen deprivation therapy for unfavorable-prognosis disease).”
Title: Grade Group 1 Prostate Cancer Outcome by Biopsy Grade and Risk Group
Authors: Neal A. Patel, Daniel A. Barocas, Daniel W. Lin, Xian Wu, David Green, Kevin H. Kensler, Jonathan Shoag, Bashir Al Hussein Al Awamlh.
You can read the Full Article in JAMA Oncology.

More posts featuring Miguel Bronchud on OncoDaily.
{kind=link}
-
Challenging the Status Quo in Colorectal Cancer 2024
December 6-8, 2024
-
ESMO 2024 Congress
September 13-17, 2024
-
ASCO Annual Meeting
May 30 - June 4, 2024
-
Yvonne Award 2024
May 31, 2024
-
OncoThon 2024, Online
Feb. 15, 2024
-
Global Summit on War & Cancer 2023, Online
Dec. 14-16, 2023