
Myeloma drugs – Dosing and schedule by Vincent Rajkumar on Twitter
Myeloma drugs — Dosing and schedule
What I do in practice
Dex: 40 mg once a week age <70; 20 mg if age >70 or frail
Stop Dex at around one year if good response.
Days 1-4, 8, 15, 22 schedule for 1st cycle only in cast nephropathy; or VDT-PACE type regimen.
Velcade:
Once a week and SQ is my default.
Twice a week for 1st cycle only in acute in cast nephropathy, or with VDT-PACE type regimen.
Revlimid:
25 mg standard. But reduce starting dose to 10-15 mg for the following groups: elderly, frail, patients with body weight less than 60kg, renal failure, and patients of Asian or South Asian descent.
Maintenance dose: 10 mg max.
Pomalidomide:
2 mg standard.
Not 4 mg.
Carfilzomib:
Once weekly. Not twice weekly.
Usual schedule: 56 mg/ m2 days 1, 8, 15 of 28 day cycle. (First cycle first dose 20 or 27 mg/m2)
Bispecifics:
I don’t know the answer. But it is definitely not every 2 weeks continuous. I think we are going to deescalate quickly after response with all of these drugs for safety. And either stop or reduced frequency even more once once good response is achieved.
Cyclophosphamide:
300 mg/m2 oral. Once a week. Depending on counts either every week or more often I do 3 weeks on and one week off.
I find KCd and VCd two underutilized highly effective regimens for relapsed MM.
These doses are less than what was published in the original trials based on subsequent information on safety and efficacy. More here. onlinelibrary.wiley.com/doi/abs/10.100

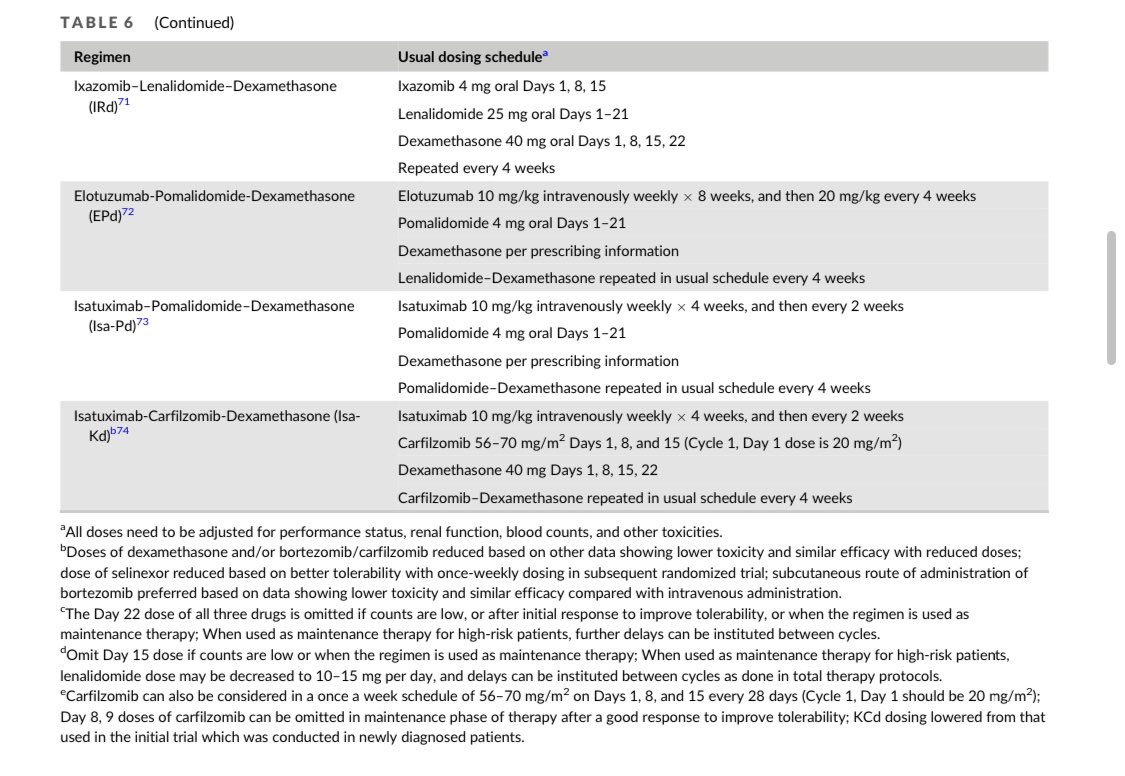
Important: Chemotherapy doses and schedules are complex and these are just concepts and suggestions. You have to verify everything when prescribing. You have to individualize. And modify based on patients characteristics at baseline and on follow up.
Bone prophylaxis. I hardly ever use denosumab.
Zoledronic acid is default. Once a month for a year then every 3 months for 1-2 years and stop. Restart at once every 3 months at relapse. Slow down/stop after response achieved.
If denosumab is used, give monthly for 2 years and stop. After stopping, one dose of zoledronic acid should be given to prevent rebound.
Source: Vincent Rajkumar/Twitter