
Talha Badar: Rx of Lower risk MDS, non del 5q, failing ESA/luspatercept
Talha Badar, Assistant Professor at Mayo Clinic Comprehensive Cancer Center shared a thread on X:
“Weekend Review Thread:
Rx of Lower risk MDS, non del 5q, failing ESA/luspatercept
Huge unmet medical need!!
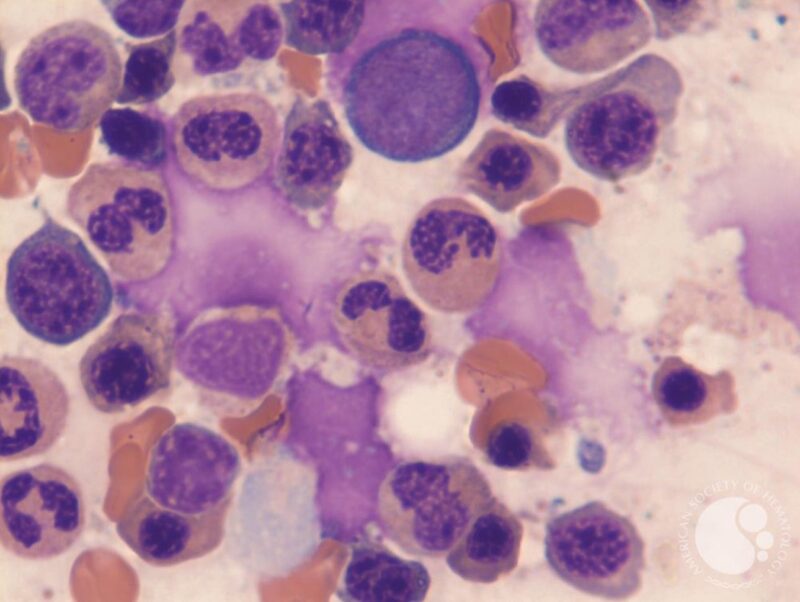
ASH-image of MDS-RS
QOL in LR-MDS failing ESA
While low risk disease, has significant impact on quality of life and mobility. More so in females, pts with co-morbidities and higher transfusion burden. (read more)
Lenalidomide for LR-MDS (non del 5q) failing ESA and TD
PIII placebo controlled study, 239 pts enrolled
RBC-TI ≥ 8 weeks was achieved in 26.9% and 2.5% of pts in the lenalidomide and placebo groups, respectively (P < .001)
Median duration of RBC-TI with lenalidomide was 30.9 weeks (95% CI, 20.7 to 59.1).
Lenalidomide did not negatively effect QoL. (read more)
HMA therapy for LR-MDS
Modified doses of HMA therapy is being used for LR-MDS refractory to first-line therapies.
Better responses are seen in pts with less transfusion burden. (read study 1, study 2, study 3)
Outcome of LR-MDS (non del5q) after ESA failure
Prior to luspatercept, common therapies were lenalidomide, and HMA
Five-year AML cumulative incidence was 20.3%, 20.3%, and 11.3% for those receiving HMAs, LEN, and MISC, respectively (P = .05).
Five-year OS for patients receiving HMA, LEN, and MISC was 36.5%, 41.7%, and 51%, respectively (P = .21). (read more)
Roxadustat (HIF inhibitor) for LR-MDS non del5q
PIII MATTERHORN trial examining roxadustat did not meet its primary end point. (read more)
Splicing modulator in LR-MDS post ESA
Oral SF3B1 modulator H3B-8800 in myeloid neoplasms, after initial promising results couldn’t advance further due to toxicity. (read more)
IDH1 inhibitor in MDS
IDH1m present in 3-5% of pts with MDS, IDH1i received approval for management of MDS based on data.
Encouraging responses seen in HMA refractory pts, however this is only present in small number of MDS patients. (read more)
LR-MDS non del5q post ESA
Telomerase inhibition has shown promising efficacy in myeloid malignancies.
imetelstat, a competitive inhibitor of telomerase
PIII trial evaluated imetelstat vs placebo, LR-MDS with transfusion dependence.
40% achieved PI, transfusion independence for 8 wks or more.
Most common G3 adverse events were neutropenia and thrombocytopenia
Findings are very promising, hoping drug approval soon!
LR-MDS non del5q, TD, failing ESA/luspatercept.
Conclusion
- Lower risk MDS, non del 5q, failing ESA/luspatercept is a huge unmet medical need!!
- Most of these pts are elderly with co-morbids and ineligible for intensive therapies.
- Response to HMA in elderly with high transfusion burden, secondary hemosiderosis are modest.
- I always find difficulty in managing toxicity sec to lenalidomide in elderly with MDS
- IDH1i is efficacious but present in very small subset of MDS.
- Imetelstat phase III data is promising, anxiously waiting its approval.”
Source: Talha Badar/X
OncoDaily
Dr. Talha Badar, MD, is a specialist in Hematology Oncology based in Mayo Clinic, Jacksonville, Florida. His primary areas of expertise include Leukemia, particularly Acute Myeloid Leukemia (AML), Myelodysplastic Syndrome (MDS), Acute Lymphoblastic Leukemia (ALL), and Bone Marrow Transplantation. Over his career, he has actively contributed to clinical research and clinical trials.