Rafael Fonseca: The clinical development curse against venetoclax for t(11;14) multiple myeloma.
Rafael Fonseca, the Chief Innovation Officer at Mayo Clinic, Arizona, recently tweeted on X/Twitter:
”The clinical development curse against venetoclax for t(11;14) MM (multiple myeloma) – How CANOVA was reported and why it is still critical patients with the t(11;14) have access to Ven.
Ven is a “game changer” – a hill I am ready to die on. The first and most effective targeted therapy for MM with t(11;14). It is long overdue we have unfettered access to it for patients that need it.
CANOVA is a registration Phase 3 study comparing Ven-d vs. Pd in RR t(11;14) MM. The very specific hypothesis to keep in mind is whether ven can be proven to be superior to Pd in t(111;14) RR MM patients who have received at least 2 prior lines of Rx.
Is this question important? Hardly. Most people who are administering Ven now do so after Pom failure- I would argue it should be used earlier. But this question is a false clinical dichotomy. It exposes clearly the failure of regulatory pathways.
If Ven is a game-changer, why was it NS? Trial design and execution remains a challenge for Ven. Perhaps the trial should have been VenPd vs. Pd. Nevertheless, one would imagine the great activity we see in the clinic is such that this would be a “slam dunk.”
The global trial was small in size, but even then, we would have predicted a large difference. Interestingly (in a negative way), many pts came off the study early on, even without disease progression (MD/pt preference). I suspect many were just looking for access to Ven.
In the supplementary data, one can see that many more got Ven post progression: 3 (2%) vs. 24 (19%). Even then, one would have predicted significance. The ITT curves show clear separation, even though the stats are NS. I would say it is highly likely that difference exists.
A post-hoc analysis shows that by adjusting for criteria for progression (as should have been done), the difference is clear. Context matters! Anyone arguing that the primary outcome, as reported, describes Ven is not familiar with Ven for t(11;14) MM.
Even the OS curve favors Ven, and the study is ongoing (TBD).
What are other potential confounders? The patient in the Ven arm had more lines of treatment than those in the Pd arm: 3 (2–8) vs. 2 (2–8).
At the time of the trial design, the dose was less clear. We used to treat with up to 800-1200 mg daily! Now, we think 400 is a better and safer dose. Ven is very well tolerated- the number one complaint by patients is pill burden, so 400 is even better.
Infections/related deaths were higher with Ven, so we have to be careful. All deaths occurred in the absence of IVIg replacement. N. van De Donk has now shown the importance of the replacement of IgG with bispecifics, and Ven should be considered. Antibiotic prophylaxis too.
Other aspects in favor of Ven, beyond the adjusted PFS post-hoc reported. The TTNT, OR, and OS seem to all point in the right direction. It is all consistent with what we now have as extensive clinical experience with this drug.
I would argue Ven is a far superior drug for t(11;14) than elotuzumab who beat Pd and is perhaps just as good and a great partner to CD38 abs (isa and dara). A strict analysis of the available published data would suggest this is wrong.
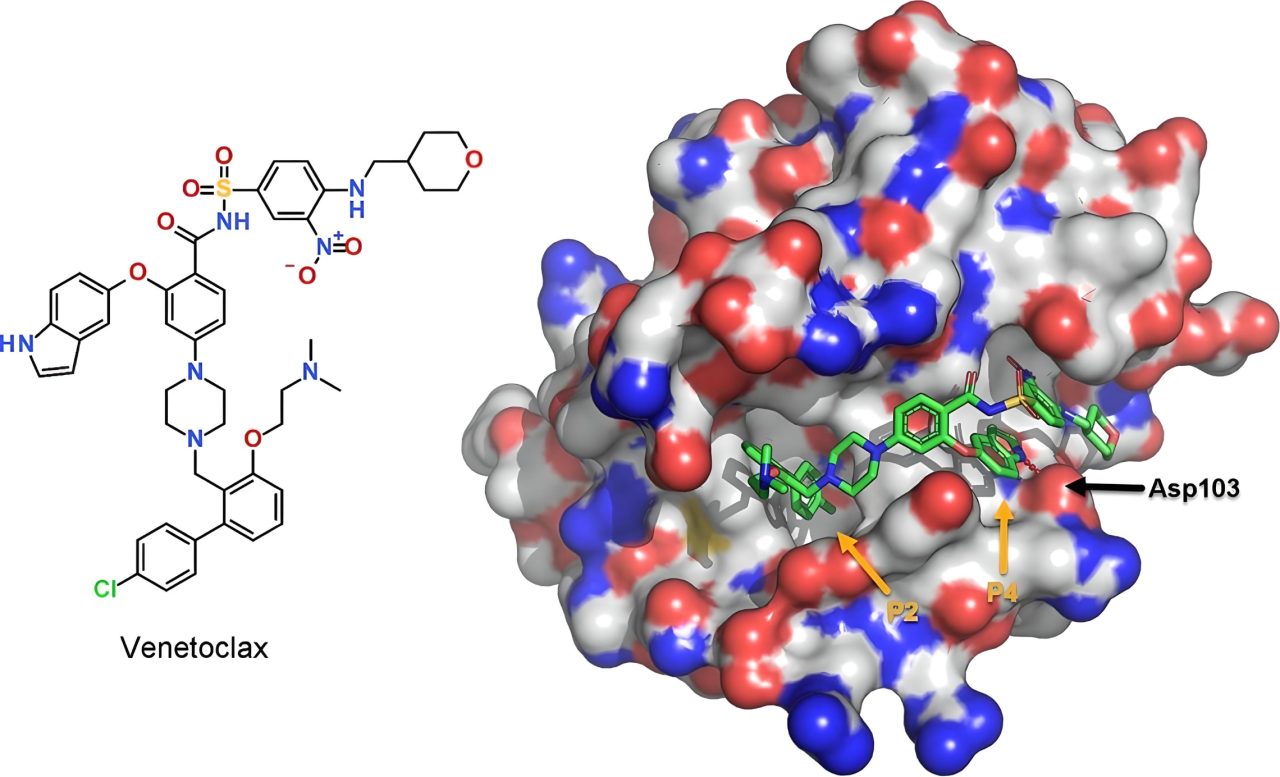
So why is ven a game changer? First, the biology is impeccable. Many labs have shown its MOA (bcl-2 in t(11;14) MM vs MCL-1 in others). MM with t(11;14) is a different entity and one for which we have this targeted approach. I will not cover this in more detail here.
Many of us have used empirically Ven in t(11;14) MM and AL with great success. What does this mean? Patients with no further options have gone on to survive for several additional years when Ven was their last chance.
With dex only we have had about 2 years of disease control but sometimes 5 or more. These are much more than anecdotes – real patients with extended lives. The data in combination, is impressive. The first report by Nizar Jacques Bahlis shows its high efficacy. A cascade plot that is perfect is a square. This one for the combination of Dara-Vend (green on the left) is almost a square for those with t(11;14)!
More importantly, the PFS at 5 years for those in the 400 mg (reported at IMS 23) is close to 70%. No MM regimen has ever done that! It can be combined with PIs as well.
Not to point fingers, but all of this could have been averted with an original proper design for BELLINI. If we had a Phase 3 of Bor-Ven-d vs Bor-d, limited to those with t(11;14). The drug would be approved & available. This is why proper clinical trial design is critical.
Trials from a scientific perspective are merely one more experiment. From a human perspective these experiments involve many lives, many years and often costs hundreds of million of dollars.
In summary, Ven is a game changer but we still cannot extract the diamond from the rough. The additional wait will result in lost lives, unfortunately. Many will continue to prescribe, but the majority of oncologists will just hear “It could not show significance in CANOVA.”
What additional trials would be of interest?
– Daratumumab-ven-dex vs ANDROMEDA for t(11;14) AL
– GRFFIN or MASTER where ven replaces len in t(11;14) MM
– MAIA vs MAIA modified (ven replacing len in TIE)
– Ven maintenance and consolidation for t(11;14)
Will I continue to prescribe Ven for t(11;14) MM/AL? Resounding yes. I reject the notion that the results of CANOVA can describe the putative clinical benefit of Ven for t(11;14) MM. Academic centers, pt support organizations, and Pharma need to work to get ven to patients.
Congratulations to Dr. Marivi Mateos, Nizar Jacques Bahlis, J Kauffman, and many others, including AbbVie. But we still need to get there. For more information click here.
A link to the biology of t(11;14) and also to the first Tweet. Finish.”
Source: Rafael Fonseca/Twitter