
Piotr Wysocki: Cetuximab monotherapy maintenance after FOLFIRI may not be the optimal choice but can be considered in selected mCRC patients
Piotr Wysocki, Professor of Medicine and Head of the Department of Oncology at Jagiellonian University Hospital, shared on LinkedIn:
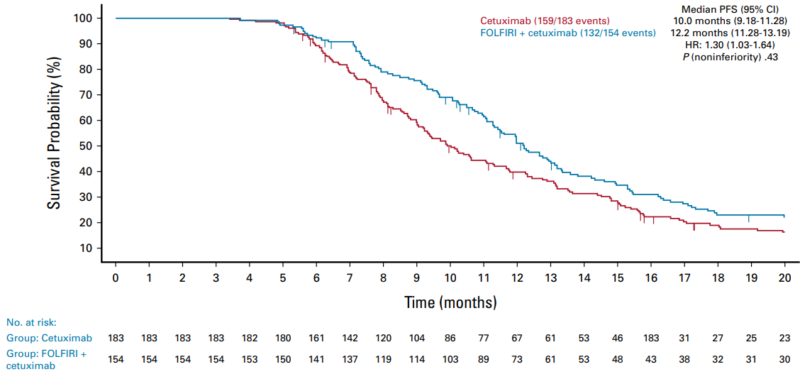
“A phase III open-label study (ERMES) has evaluated the role of single-agent maintenance with cetuximab within first-line treatment in advanced colorectal patients. The study enrolled 606 (RAS/BRAFwt) patients who were randomized in a 1:1 ratio to (A) standard chemotherapy (FOLFIRI+cet – 5-fluorouracil+leucovorin+irinotecan combined with cetuximab) given until progression or to (B) eight cycles of FOLFIRI+cet followed by maintenance with cetuximab alone. The coprimary endpoints were a non-inferior progression-free survival (PFS) in the modified per-protocol (mPP) population (at least 9 cycles of FOLFIRI+cet) and a lower incidence of grade G3-4 adverse events (AEs) for arm B compared with arm A.
With the median follow-up of 22.3 months, the PFS in the mPP was 10.0 and 12.2 months for cet maintenance and continuous FOLFIRI+cet, respectively (P of noninferiority = .43). In the intention-to-treatment (ITT, at least one cycle) the PFS was 9.0 versus 10.7 months (P =.39). The overall survival was 35.7 versus 30.7 months (P = .119) and 31.0 versus 25.2 months (P = .32) in the mPP and ITT population, respectively. Maintenance therapy with cetuximab was associated with a much lower incidence of G3-4 AEs than in the continuous FOLFIRI-cet arm (20.2% v 35.1%).
The ERMES study did not demonstrate noninferiority of maintenance with cetuximab alone, which cannot be assumed as a standard approach in clinical practice. However, it may represent an interesting option in patients demonstrating poor tolerance of the FOLFIRI+cet combination.
These results are not surprising since many earlier studies and cohort analyses suggested that cetuximab monotherapy was insufficiently active as maintenance in early-line settings.
In my daily practice, I often use a de-escalation strategy in patients achieving disease control with FOLFIRI+cet (after 3-4 months), which is based on the cetuximab+irinotecan combination. This combination was evaluated 20 years ago by David Cunningham et al. (NEJM 2004;351:337-345), who demonstrated its significant superiority over cetuximab alone regarding responses and time-to-progression (in patients unselected for RAS, BRAF status). Getting rid of a 46-hour 5-FU infusion and offering the patients biweekly 2-hour visits is very well received by the patients and still allows for much better disease control than cetuximab monotherapy.”
Read further.
Source: Piotr Wysocki/LinkedIn