
Michael Shusterman: Just a reminder about why we should NOT use bolus 5-FU in combination with the infusion
Michael Shusterman, Medical oncologist and Clinical Assistant Professor of Medicine in the Permutter Cancer Center at NYU Langone Hospital, shared a post by Mark Lewis, on X:
“Just a reminder to bring back this educational thread about why we should NOT use bolus 5-FU in combination with the infusion. Still a long way to go as many trials and oncologists are still using the bolus in the metastatic setting.”
Quoting Mark Lewis‘s post:
“WHY I (ALMOST) NEVER BOLUS 5-FLUOROURACIL I’ve been pondering this thread for a while but it’s become more urgent in light of another looming chemo shortage <deep sigh>, this time with an imminent dearth of THE foundational drug of GI oncology: 5-fluorouracil, or 5-FU.
An attending of mine from fellowship said ‘every patient with GI cancer deserves to receive FOLFOX’ and, while that may have been a statement of its time (I trained 2009-2012, pre-KEYNOTE 177!) it still has the ring of truth today
So, while we should ALWAYS be thoughtful prescribers of chemotherapy (primum non nocere, anyone?), if we have a finite supply of 5-FU, and some other cytotoxic drugs are likely only active with a fluoropyrimidine backbone, we should be particularly parsimonious with its use.
In mFOLFOX6 the ambulatory infusion of 5-FU is 2400mg/m2 and the bolus is 400mg/m2 so the bolus comprises ~14% of the entire drug usage (put another way, we can enable 1 extra pump fill for every 6 boluses held).
And while FOLFOX (whether FOLFOX4 or 6) has been the workhorse regimen in mCRC for decades, we have data from the pre-oxaliplatin era (EORTC 40952 & even Moertel in 1972!) that slow(er) infusion had similar activity in the metastatic setting (but could not deduce additive effect)
Much more recently, the abstract below caught my eye at ASCO GI earlier this year (GI23) ‘The use of a 5-FU bolus was not associated with OS (HR 0.98; 95% CI 0.91-1.06; p = 0.64).’ You can’t fit a laser pointer between these survival curves.
Stated more simply, why bolus a drug over 15 minutes that is then going to be in circulation for at least 46+ hours? (You also, in theory, don’t need leucovorin to lengthen the half-life of bolus 5-FU if infusional alone is being used)./Article./
1) ask what the 5FU bolus is adding (or not) to your GI onc regimens and if you can possibly omit it
2) ask, relatedly, if leucovorin is needed
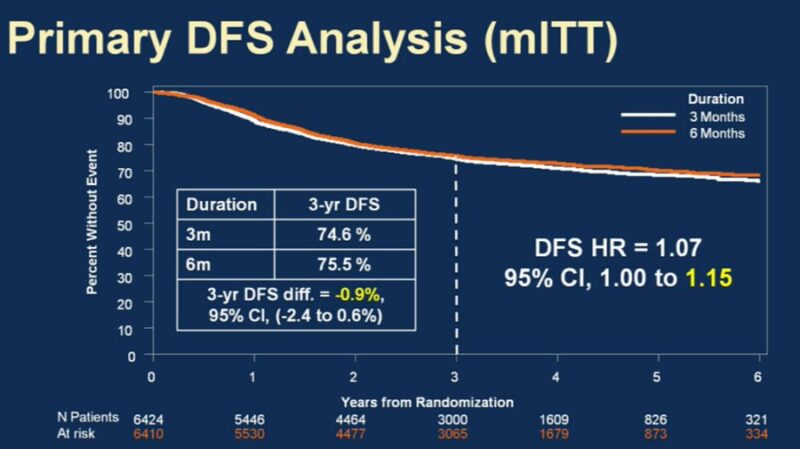
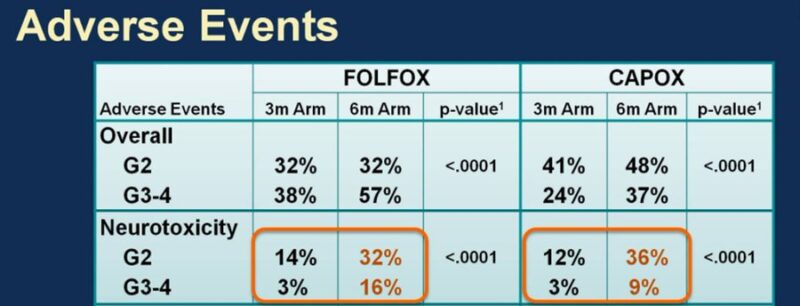
3) consider capecitabine when appropriate and don’t forget IDEA’s risk strata/durations
4) talk to your pharmacists :)”
Read further.
Source: Michael Shusterman/X and Mark Lewis/X
Mark A. Lewis is the Director of Gastrointestinal Oncology at Intermountain Healthcare in Utah, the Co-Chair of adolescent & young adult (AYA) oncology in the SWOG cooperative group, and the Vice President of American Multiple Endocrine Neoplasia Support. Dr. Lewis is also a well-known patient advocate and social media influencer.
About OncoDaily
OncoDaily was founded in 2023. It is a US-based oncology media platform, which features the latest news, insights, and patient stories from the world of oncology. Within short period of time it became one of the leading oncology media platforms globally.
OncoDaily gathers content from various sources, including social media posts from renowned oncologists from all over the world, news from oncology societies and cancer centers, patient and survivor stories, and career-related information for professionals.
The mission of OncoDaily is to empower patients, survivors, and professionals with the knowledge and inspiration they need to fight cancer. The motto of OncoDaily is “Cancer doesn’t take a day off – neither do we.”